
|

|
|
|
|
|
This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included.
Type 2 Diabetes Revisited: Why Blood Sugar Is Not the DiseaseA Three-Level Model from Glucose Control to Systems Restorationby Richard Z. Cheng, MD, PhD
Highlights
Why This MattersFor decades, type 2 diabetes has been defined-and treated-as a disorder of elevated blood glucose. Yet large clinical trials have shown a striking and uncomfortable truth: Lowering blood sugar does not reliably prevent the most serious outcomes of diabetes-heart attacks, strokes, or death. This raises a fundamental question: What if glucose is not the disease-but a marker of a deeper systemic failure? AbstractType 2 diabetes mellitus (T2DM) is conventionally managed as a disorder of hyperglycemia. However, major clinical trials such as ACCORD, ADVANCE, and VADT demonstrate that intensive glycemic control does not consistently reduce macrovascular complications or all-cause mortality. These findings indicate that hyperglycemia is not the sole driver of diabetic pathology. From a systems medicine perspective, particularly within Integrative Orthomolecular Medicine (IOM), T2DM is a systems-level disorder involving oxidative-reductive imbalance, mitochondrial dysfunction, micronutrient depletion, hormonal dysregulation, and environmental influences. A central and underrecognized mechanism is that hyperglycemia impairs cellular uptake of vitamin C via competitive inhibition at glucose transporters, leading to functional intracellular deficiency despite normal plasma levels. This represents a transport-level "pseudo-deficiency" that contributes to oxidative stress, endothelial dysfunction, and vascular complications. We propose a three-level model of T2DM management:
While metabolic therapies represent a major advance, they do not fully restore intracellular and systemic biological function. IOM Systems Medicine represents the next necessary level of intervention. 1. The Clinical Paradox of Glycemic ControlDespite decades of emphasis on lowering blood glucose, major clinical trials have shown limited impact on hard outcomes. Intensive glycemic control:
Why do complications persist even when glucose is controlled? Because glucose is a downstream signal-not the upstream cause. 2. Type 2 Diabetes as a Systems-Level DisorderT2DM is more accurately understood as a systems disease involving:
These processes converge through disruption of the oxidative-reductive (redox) system, forming a shared biological terrain that drives disease progression. 3. Metabolic Medicine: Role and LimitationsLow-carbohydrate and ketogenic diets represent a major advance beyond conventional glucose-centric care. They:
However: Metabolic control does not equal biological restoration. Even with improved glucose markers, key dysfunctions may persist:
Metabolic therapy is a transition layer:
4. Hyperglycemia-Induced Functional Vitamin C DeficiencyA Central Mechanism of DiseaseGlucose competes with vitamin C for cellular transport. Under hyperglycemic conditions:
This creates a functional deficiency-a transport problem, not an intake problem. A New PerspectiveThis phenomenon is part of what we describe as the Insulin-Cortisol-Vitamin C (ICV) axis, linking glucose metabolism, hormonal signaling, and intracellular nutrient delivery. In effect: Diabetes may represent a state of "cellular scurvy." 5. A Self-Reinforcing Disease LoopHyperglycemia → ↓ intracellular vitamin C → ↑ oxidative stress → ↑ insulin resistance → worsening hyperglycemia This feedback loop helps explain why complications persist despite glucose control. 6. The IOM Nutrient Demand PrincipleA core principle: As disease burden increases, nutrient demand increases. In T2DM, demand rises due to:
Standard dietary intake may be insufficient to restore cellular function. 7. Key Nutrient Deficiencies in DiabetesCommon deficiencies include:
These are not secondary findings-they are core drivers of dysfunction. 8. Hormonal and Environmental DriversMetabolic dysfunction is further amplified by:
These factors interact with the redox system and shape the biological terrain. 9. Toward a Systems Therapeutic ModelEffective care must integrate:
10. Three Levels of Diabetes Management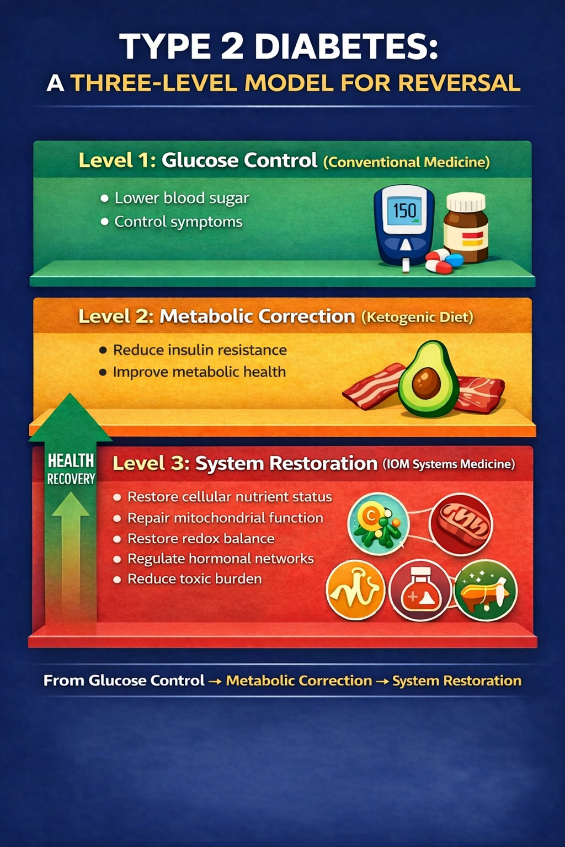
Fig. 1. A three-level model for type 2 diabetes mellitus (T2DM).
Level 1 - Glucose Control (Conventional Medicine)
Level 2 - Metabolic Regulation
Level 3 - IOM Systems Medicine
Key insight: Hyperglycemia is both a marker and a driver of systemic dysfunction. 🔥 Positioning StatementLow-carbohydrate and ketogenic therapies represent a major advance in diabetes care. But they are not the endpoint. The next step is not better glucose control-
ConclusionType 2 diabetes is not simply a disease of high blood glucose. It is a systems-level disorder characterized by:
While metabolic approaches address key drivers, they do not fully restore biological function. IOM Systems Medicine provides the next step: systems restoration. OMNS TakeawayFocusing only on blood glucose misses the core biology of diabetes. Effective care must address:
Scientific SourceA full-length scientific version of this article has been published as a preprint: Cheng RZ.
Orthomolecular MedicineOrthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org Find a DoctorTo locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource. Editorial Review Board:
Jennifer L. Aliano, M.S., L.Ac., C.C.N. (USA)
Comments and media contact: editor@orthomolecular.org OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication. To Subscribe at no charge: https://www.orthomolecular.org/subscribe.html To Unsubscribe from this list: https://www.orthomolecular.org/unsubscribe.html |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
