|

|
|
|
|
 Back to 1994 3rd Quarter Table of Contents
Back to 1994 3rd Quarter Table of Contents
Presented at the 23rd Annual Nutritional Medicine Today Conference, April 29, 1994, Vancouver, Canada. More than 40 years ago, Abram Hoffer, M.D., Ph.D., and Humphry Osmond, M.D., introduced a concept of how the brain works at the molecular level and how defects in this complex system relate to schizophrenia.. This early work opened up the field which was later called biological psychiatry, or Orthomolecular medicine.1,2 Because the traditional psychiatric medical model is not working for many people, interest has increased in the Hoffer/Osmond concepts. The present psychiatric model provides therapeutic benefit for a number of crisis disorders, but for many chronic metabolic conditions of the brain, in which a complex milieu of interlocking biochemical and physiological processes are at work, this approach has significant limitations. An expanded therapeutic model, derived from the pioneering brain biochemistry work of Drs. Hoffer and Osmond is now being tested in clinical and laboratory research. This expanded model is based upon an understanding of the duration, intensity and frequency of mental health symptoms and their relationship to brain biochemical patterns. For the past four years my colleagues and I have employed a questionnaire which evaluates symptomatologies on a patient-specific basis. Leo Galland, M.D., developed the term "patient-centered diagnosis" to describe this method of assessment, using the patient as his or her own internal control, examining the individual's functional physiological ability without the limitation of disease attribution.3 The three page Metabolic Screening Questionnaire asks the patient to rank organ-specific intensity, duration and frequency of symptoms on a scale of 0 to +4. This questionnaire, which was developed from the Cornell Medical Index, has been used to evaluate several thousand people during the past four years. We have found the data from this questionnaire correlate very well with the Medical Outcome Survey Short Form 36 developed by the New England Medical Center, which has been validated by extensive research defining it as an effective quality-of-life assessment tool.4 We have found the Metabolic Screening Questionnaire to be much less time-consuming to fill out and that there is a correlation of approximately 0.8 between the two questionnaires. The relationship between the information derived from this questionnaire and nervous, immune, endocrine and gastrointestinal system dysfunctions, led to the hypothesis that many chronic mental and physical health problems are related to the accumulation of metabolic toxins. Examples of these metabolic toxins include the neurotoxins adrenoleutin and adrenochrome, which are derived from epinephrine. There are literally thousands of molecules, both native to human physiology and of exogenous origin, that could impair neurobiochemical function at some concentration. The Relationship between Toxins and Nervous System Function There is a very complex relationship between the
concentration of various substances within the neuron and the function of the
nervous system. The concentration of these substances changes throughout the
day, with one's circadian rhythms and age, experiences, stress level,
environment, drugs and alcohol consumption, the functional status of his or her
gastrointestinal and hepatobiliary systems, and the diet. The analysis of the
metabolite/toxin patterns can be accomplished using pattern recognition,
sophisticated mathematical methods and computer technology. What is emerging is
the recognition that a number of brain disturbances result from the accumulation
of various patterns of neuro-active substances of both endogenous and exogenous
origin.
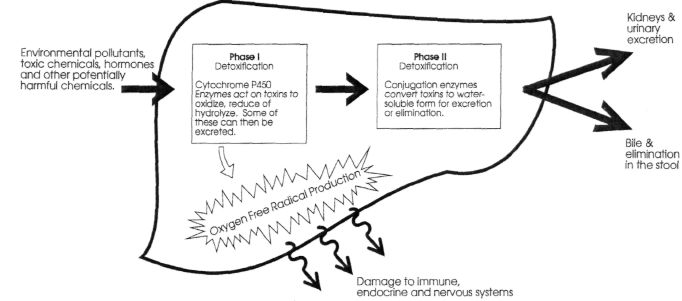
Figure 1. Detoxification in the Liver The body's ability to rid itself of toxic substances from
the environment is dependent upon proper function of the liver. In the liver,
detoxification occurs in two general phases. Each of these phases may be reduced
or enhanced in activity, depending upon availability of critical
nutrients. Many neurotoxins in systemic circulation are detoxified by
the liver. There are two metabolic steps by which the liver transforms most of
these toxic "foreign" substances into nontoxic derivatives which are excreted
with the bile (in the feces) and in the urine. These steps are shown in Figure
1. These substances may be of exogenous origin, originating in the external
world, or they may be endogenously produced, having built up in the brain or
other tissues due to an error of metabolism.5 The first step in hepatic detoxification involves the
cytochrome P450 mixed-function oxidase super-family of enzymes. There are many
different types (isozymes) of cytochrome P450 with abilities to remove different
chemicals from the bloodstream by an oxidative process. The cytochrome P450
family of enzymes produces in the liver an intermediate series of compounds
called oxygenated metabolites, or biotransformed intermediates, which can be
even more toxic than the original substances. Fasting as a method of
detoxification can increase the level of biotransformed intermediates in the
body. Some individuals continue to get more severe symptoms as they fast,
because their liver's Phase II enzyme systems cannot keep up with the load of biotransformed intermediates with which they
are presented. In Phase II of detoxification, the oxygenated or
biotransformed intermediates are converted to nontoxic byproducts that can be
excreted. They go into the bile if they are higher molecular weight toxins, or
into the urine if they are of lower molecular weight. This second stage is
called the conjugation stage of detoxification. The liver has six separate
pathways for converting these transformed intermediates to nontoxic derivatives.
They include amino acid conjugation, glucuronidation, acetylation, sulfation,
sulfoxidation and glutathione conjugation. The ability of the liver to detoxify
toxic substances, therefore, depends upon the activity and balance of both the
Phase I and Phase II enzyme systems. If they are not working in balance, toxins
which can alter brain chemistry and behavior can
accumulate.6 In our research, we have found that both Phase I and Phase
II detoxification systems can be modified through specific nutritional
intervention. If a person is undernourished, then he or she is less able to
detoxify various toxins. If you give inadequately nourished individuals the
right balance of nutrients (at required doses that may be higher than the Recommended
Dietary Allowance), their detoxification ability and symptoms of many functional
neurological disorders improve.7 The origin of many toxic substances with which the liver
must cope is the gastrointestinal tract. Hundreds of substances which originate
from bacterial action in the gut cross the GI mucosal border in apparently
healthy people, and all of these substances must be detoxified by the liver.
Therefore, an individual's ability to protect against brain-active substances
depends upon the status of the intestinal flora, GI mucosal function and hepatic
detoxification ability.8 A permeable GI mucosa is known as a
leaky gut. When the gut becomes leaky, more substances are delivered to the
liver, and if the liver's functional ability to detoxify is impaired, more
metabolically active substances are delivered through the bloodstream to other
tissues, including the brain.9 In a study of brain-injured children at the Institutes for
the Achievement of Human Potential in Philadelphia, Pennsylvania, we have found
that many of these children have an impaired gut/liver detoxification system.
They are, therefore, exposed to more toxins originating in their gut,
potentially overloading their liver detoxification system, resulting in an
adverse impact on their brain chemistry. Pattern Recognition Analysis and Gut/Liver
Function Wayne Matson, Ph.D., vice-president of ESA, Inc., in
Massachusetts, has developed a technology which makes it possible, using a very
small volume of plasma, urine or cerebral spinal fluid, to analyze
simultaneously more than 5,000 metabolites. Through cluster analysis of these
metabolites, certain patterns have been identified, making it possible to design
specific nutritional therapies to improve gut and liver detoxification function.
This technology has been used as part of the program at the Institutes for the
Achievement of Human Potential to differentiate the metabolite clustering of
individuals with midbrain or cortical brain injuries from that of individuals
who have autism or epilepsy.10 From these observations we have been exploring how various
brain metabolite patterns relate to the gut/liver connection. We have confirmed
that various factors, such as medi- cations, alcohol, allergies, autoimmune disorders,
dysbiosis, environmental toxins and substance abuse all impact the barrier of
defense called the gut mucosa." When the gut mucosa is disturbed, permeability
increases, facilitating the passage of various substances to the liver. Ten
percent of the liver by weight is composed of cells called Kupffer cells, which
are imbedded lymphocytes; therefore, the liver is in part an immune system
organ. When the Kupffer cells of the liver are activated by antigens passing
across the permeable GI mucosa, they trigger the release of chemical messengers,
lymphokines and cytokines, represented by interleukins 1, 2, 6, 12, tumor
necrosis factor and gamma interferon. 12 These substances travel to
target tissues, including the blood/brain barrier, altering cellular function.
This altered function results in modification of biological response in the
immune, endocrine and nervous systems. Many chronic symptomatologies may be a
manifestation of the continued chronic release of cytokines which, in a sense,
represent the cellular messengers, resulting from a continued "toxic"
insult. Oxidative Stress and Neurobiochemistry Secondarily, when the liver is engaged in trying to
detoxify nervous system-active toxins and drugs, it also produces oxidant stress
byproducts, such as superoxide, hydroxyl radical, hydrogen peroxide and singlet
oxygen, which are very reactive molecules. These molecules react rapidly with
structural protein, enzymes, DNA or membrane lipids, resulting in nonspecific
tissue damage. Therefore, an overly active detoxification system, due to an
abundance of substances the liver has to detoxify, enhances oxidative stress,
which requires more antioxidant protection. The principal damaging effects of
oxidative stress are manifest in oxygen-sensitive tissues, such as the brain,
kidneys, heart, blood and lungs.13 In our research with brain-injured children, when we
examined whole blood reduced glutathione levels, we found that many of them had
very low levels of this important antioxidant which circulates in the blood.
Whole blood reduced glutathione is reflective of the redox (reduction/oxidation)
potential of the whole body, and a low level of blood glutathione indicates the
body is under considerable oxidative stress. In other words, many of these
brain-injured children either were not able to synthesize glutathione, or they
were under high oxidative stress that was causing depletion. Therefore, we
concluded, children who had sustained brain stem, cortical or midbrain injuries
in general had very high levels of oxidative stress, which meant that toxins
(oxidants) were affecting their brain chemistry. Protection against these
oxidant stress reactions is provided by antioxidants. The need for these
protective substances, which include vitamins C and E, bioflavonoids, and the
enzyme-activating minerals zinc, copper, manganese and selenium, may be much
higher in an oxidatively stressed individual. Another condition which is associated with very low levels
of whole blood reduced glutathione and high levels of oxidative stress is AIDS
encephalopathy. It is believed that the condition that damages the brains of
terminal AIDS patients is, once again, the depletion of antioxidant protection,
such as glutathione, due to high oxidant stress load.14 When
examining data from studying the brain-injured children, we concluded there
might be something significant about oxygen toxicity, or free radical toxicity,
in these children. Paradoxically, the time when the brain is most subject to
oxidative stress is the time when it has the least oxygen available. Children
who suffer from various neurological problems generally exhibit shallow
breathing, little activity, compressed chest, poor posture and low oxygen
tension. If they have had some kind of brain injury, they might also have
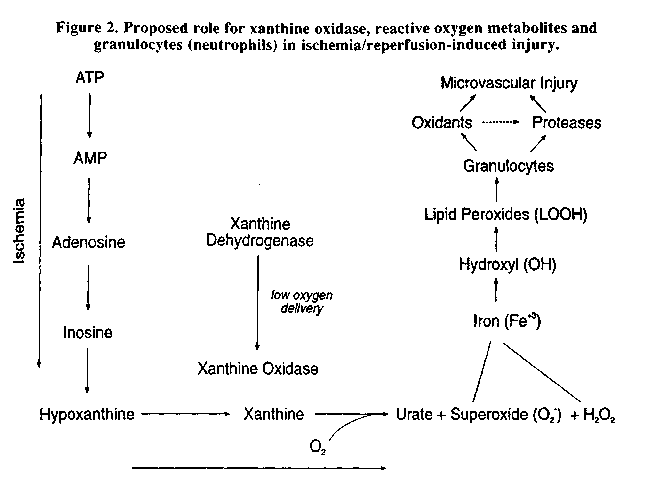
suffered vascular damage that prevents proper oxygen delivery. If the brain is deprived of oxygen, the mitochondria in the
neurons cannot produce energy properly, and oxygen becomes a limiting nutrient.
When oxygen becomes a limiting nutrient to the brain, the brain cannot build its
energy-carrying intermediates, such as adenosine triphosphate (ATP). If the
brain can't build ATP, that substance is quickly broken down into a number of
other substances. An enzyme in the nervous system, xanthine oxidase, becomes
activated, as shown in Figure 2. The xanthine oxidase enzyme tries to clear
xanthine from the body to produce uric acid, and in doing so it creates
superoxide as a byproduct. In the presence of iron or hemoglobin, superoxide is converted into hydroxyl radical,
which quickly contributes to further damage of the brain. Therefore, the time of
lowest oxygen tension, when oxygen is the limiting nutrient in the brain, is
when the brain is under highest oxidative stress and incurs the most
damage.15 Oxygen-Antioxidant Therapy for Brain-Injured
Kids In conditions of high oxidative stress, anything one can do
to increase oxygen tension to the brain and reduce the deleterious effects of
oxygen free radicals might be considered beneficial. This includes administering
ascorbate (vitamin C), tocopherol (vitamin E), Carotenoids, bioflavonoids and
coenzyme Q10, all of which are nervous system-protective nutrients.
(Incidentally, they also protect other oxygen-rich tissues, such as those in the
heart, blood and liver.) It is important to increase oxygenation of the tissue
which, in the case of these brain-injured children, means getting them to
breathe deeply and start moving and participating in physical therapy. When the
nutritional intake includes an enhanced intake of antioxidants, and they are
exposed to exercise through a graded program of physical therapy, their
depressed glutathione levels begin to rise to normal. Many of the altered brain
neurochemicals, such as metabolites of epinephrine, dopamine and serotonin,
start to improve or normalize with such a program, because the metabolism of
dopamine and serotonin families of neurochemicals is controlled in part by the
redox potential of the nervous system. Methods of evaluating the redox potential of the nervous
system in neurobiochemistry have only recently begun to be utilized. In doing so
we have seen that altered neurochemicals often relate to the inefficient use of
oxygen or the unavailability of redox agents like vitamin C, vitamin E,
carotene, bioflavonoids and coenzyme Q10. This new method of evaluation may
provide a whole new fundamental methodology for modifying nervous system
function in individuals who have altered neuronal oxidation-reduction
function. In the nervous system, the power of the neuron is generated
by the same type of metabolic process that generates energy for the rest of the
tissues of the body, through the metabolic activity of the mitochondria. In
the mitochondria, oxygen is combined with nutrient-derived
substrates to give rise to metabolic energy. The neurons use that metabolic
energy for the synthesis and release of neurotransmitters and neurochemicals
which are transmitted through the body where they affect the modification of
organ system functions. In other words, activation of the nervous system
stimulates the process of oxidative phosphorylation in the production of
neurotransmitters and neuromodulators such as serotonin, dopamine and
noradrenaline and their metabolites, which subsequently must also be detoxified.
In fact, through their metabolic activity, the neurons are responsible for the
production and metabolism of a complex array of intermediary metabolites. If the
neurons have been subjected to chemical, oxidative or traumatic stress (from
injury or accident), altered concentrations of these metabolites develop, and
physiological process is modified. There is a relationship, therefore, between
neuronal biochemistry, detoxification mechanisms, the overall toxic load on the
body, and cognitive and emotional func- tion. If a child has sustained a brain injury resulting in
an ischemic event (a state of low oxygen tension in the nervous system), that
event increases the toxins produced as byproducts of altered neuronal
biochemistry. This may be further complicated by chronic gastrointestinal
infection (e.g., dysbiosis) and the associated leaky gut. The liver then is
exposed to other toxins it has to process, producing increased oxidative stress
reactions. The cumulative effects of all these factors can be expressed as
altered function of the nervous, immune and endocrine systems. Nutritional Modulation of Neuronal
Biochemistry Although the brain represents only 6 percent of body
weight, it consumes between a quarter and a third of the body's oxygen and blood
sugar. A very metabolically hungry organ, the brain is fueled by blood sugar,
glucose. It converts sugar into energy through the Krebs cycle in the
mitochondria, then through the electron transport chain, eventually producing
high energy-carrying intermediates such as ADP and NADPH. These are potential energy
sources the brain uses to manufacture neurotransmitters and neuro-regulators and
to power nerve depolarization which transmits electrical impulses down the
nerves. This process requires the proper use of oxygen by the neuron in its
metabolism. If oxygen is used improperly in the neuron, however, it can produce
intermediate compounds (such as superoxide or hydroxyl radical), which are
highly toxic to the nervous system. An example of this process has recently been reported by a
team of scientists in Amsterdam who deal with molecular diseases.16
The case concerned a nine-year-old boy with neuropathy of unknown origin.
When this boy was born he appeared to be normal, but as he developed he was
unable to walk. He had very poor muscle tone, and since age two he had been
confined to a wheelchair. He had undergone extensive neurological evaluation,
but the origin of the condition was not known. Finally, he was evaluated using
Phosphorus 31 Nuclear Magnetic Resonance Spectroscopy, which noninvasively
measures the metabolic energy in tissue. With the aid of this instrument, it was determined that the
boy was suffering from a breakdown in mitochondrial energy production in the
neuron as a consequence of the genetic impairment of a single enzyme, pyruvate
dehydrogenase complex IV, which represents a major metabolic control point in
the neuron. The impairment of this enzyme resulted in the production of oxygen
free radicals which were damaging the boy's nervous and muscular systems. It was
as though a metabolic wire, which we call the electron transport chain, had lost
its insulation and was shorting out. The doctors who were treating the boy concluded that the
only way to "detoxify" the free radicals and "put the insulation back" on the
electron transport chain was to give him very high doses of antioxidants. They
administered what they had concluded was a saturation level of vitamin E at 2000
IU per day. (The RDA is 15-30 IU.) After several weeks of supplementation the
ATP ratio in his resting muscle had improved considerably. Although it was still
not totally normal, it was much more nearly normal. He was producing fewer
damaging free radicals to cause alteration of his mitochondrial energy
production. Most important of all, after vitamin E therapy he was able
to walk for the first time. Neurotoxicity and Alterations in Brain
Chemistry There may be a relationship between this model and the
expression of various forms of neurological disorders as well. Several recently
published papers have described the buildup of benzodiazepine-like substances in
the blood of some individuals at concentrations high enough to alter brain
chemistry.17 Benzodiazepine is the active ingredient in diazepam
(Valium). The patients described in these articles never consumed any
diazepam-containing drugs, but their blood contained pharmacologically active
concentrations of these benzodiazepine-like substances. Where they came from is
still unknown, but it has been suggested that they may have come from the
synthesis of bacteria in the gut, alterations of the metabolism of nitrogenous
compounds in the liver, neuronal biosynthesis, or even from certain foods.
Potatoes and wheat both naturally contain very small amounts of
benzodiazepines.18 The levels in these foods, however, are too low to
account for the pharmacological concentrations of benzodiazepines found in these
patients, unless the individuals' detoxification processes for diazepines were
impaired, preventing the elimination of these substances they consumed in wheat
and potatoes. When we examined apparently healthy peo-ple's ability to
detoxify these substances, we were surprised to find individuals may differ from
one another by as much as 30-fold in their detoxification ability. People with
environmental sensitivities, who are traumatized by exposure to chemicals in
their environment, may be much more sensitive to various substances because they
can't detoxify them efficiently. These differences in detoxification ability
from one person to another may account for alterations in brain biochemistry and
behavior seen in some chemically sensitive people. It has recently been reported that there are individuals
who typically lead what seems like a normal life and then suddenly fall into a
stupor.14 When they revive they carry on normally again until they
are overtaken by the next bout of what has been described as "idiopathic
recurring stupor." Literally, this diagnosis simply means they pass out on a recurring basis
for no known reason. When a group of researchers in England took samples of
cerebral spinal fluid from a group of these patients and analyzed them by
high-pressure liquid chromatography, they found that at the time these
individuals passed out their cerebral spinal fluid contained extraordinarily
high levels of benzodiazepine-like substances. Once again, these were patients
who had never taken diazepam, but these substances built up in their nervous
system until they eventually reached a pharmacological threshold, as if the
individuals were suffering from a drug overdose. After the crisis passed, they
revived and got along fine until the substances built back up again, and then
they would have another episode. These substances were termed "endozepines,"
meaning they were diazepines manufactured by the physiological
process. All of these examples illustrate that a lot of what we may
have considered to be abnormal brain chemistry could be related to the buildup
of toxic molecules due to alterations in the body's metabolic detoxification
processes or excessive accumulation of specific substances due to impaired
metabolism. The Relationship of Neurotoxicity to Alzheimer's and
Parkinson's Diseases Many years ago, Dr. Hoffer started asking different
questions about schizophrenia. He investigated many biochemical intermediary
metabolites in brain chemistry, how they modify, alter and affect the receptor
sites and activation pathways within the brain, and how this relates to
schizophrenia. This model has now been extended into asking questions about
other nervous system disorders, such as Alzheimer's and Parkinson's
diseases. A recent report explained that Alzheimer's patients also
have mitochondrial defects that produce more free radicals that can damage
neurons.20 The formation of the neurofibrillary tangles
characteristic of Alzheimer's disease may have a genetic linkage, but not every
person with this genetic propensity develops Alzheimer's disease, which
indicates that other factors are involved as well. It has been proposed that
other mitigating circumstances which create more oxygen free radicals in
specific regions of the brain contribute to the disease. Perhaps we should be
measuring individual susceptibility factors, looking at these
intermediary substances and then tailoring nutrition to the needs of the
individual, to prevent oxidative stress of the nervous system. It has also been suggested that Parkinson's disease may be
a result of oxidative damage to the nigrostriatal neurons. The release of
excessive concentrations of oxidant free radicals in the nervous systems of
Parkinson's patients may be related not only to the genetic uniqueness of the
individual, but also to the exposure to neurotoxins from both the external and
internal environments.21 The neurotoxic events which damage neurons
in specific regions of the brain over many decades result in the loss of neurons
which finally triggers the diagnosis. Steventon in England has shown that the
ability of the hepatic detoxification systems of both Parkinson's and
Alzheimer's patients to undergo proper Phase II sulfoxidation of toxins is
impaired.22,23 As a result, both endo- and exotoxins become
potentially more neurotoxic for these genetically sensitive individuals. Over
many decades of life, the effect of exposure to toxins in these individuals who
are at risk is to reduce the "reserve" of specific neurons in the brain,
resulting first in functional neurological disorders and later in diagnosable
neurodegenerative disease. Each specific toxin may have an affinity for
different types of neurons, producing a specific molecular lesion. Based upon
the individual's unique genetic makeup and the translation of that makeup into
neurobiochemical function, different sensitivities to neurotoxicological
exposures can result. The association of xenobiotic exposure with Parkinson's
disease has been called the "environmental toxin theory" related to the risk for
the disease.24 A number of clinical reports indicate that exposure of the
brain to neurotoxins can contribute to oxidative stress reactions in the central
nervous system, resulting in premature neuronal death.25 This work
clearly indicates that protection against neurodegenerative diseases involves
identifying susceptible individuals who are poor detoxifiers. reducing exposure
to endo- and exotoxins in the susceptible individual, and then providing
antioxidant support to prevent damage by oxidative stress and nutrient intake
consistent with proper support of the hepatic detoxification systems.7 Subtle alteration in neuronal biochemistry may be
overlooked by conventional medical assessment. Once an individual has been
defined as suffering from a neurological disorder, an assumption is made that
the progression of the condition is inevitable. This assumption overlooks the
importance of asking questions about neuronal biochemistry and toxic metabolite
patterns which might be altered by selective intervention. By asking a different
question about the functional status of neuronal biochemistry, we have found
that the clinical course of many individuals may be improved. We have been exploring a variety of Orthomolecular agents
to try to modify specific metabolic patterns associated with neurotoxicity to
see if neurological function can be improved. The early results of this research
are encouraging. Functional Neurobiochemistry: A New
Approach The research we are doing, and the new technology that
makes it possible, leaves us with the question as to what insults to the nervous
system might be responsible for altered neurobiochemical function which is
observed symptomatically but which is not yet serious enough to result in a
well-defined diagnosis. Traditional neurology has presumed that without a diagnosis
an illness doesn't exist. But our research suggests there could be a myriad of
metabolic events which give rise to functional alterations in the nervous system
of the individual. Even an apparently healthy individual who "gets the blues,"
experiences mood swings or just has a "bad day" might be suffering from
transient alterations in neuroactive metabolites. Everyone has a toxic
experience at some time in his or her life a toxic headache, for example, or a
"hangover" after an overindulgence in alcohol. Until recently, we have gone
through life not knowing that biochemical derangement, due to overproduction and
underdetoxification, may be responsible for these toxicity symptoms. Our
research has begun to define reproducible metabolic patterns associated with
altered brain function, and we propose that many other mental/behavioral
problems may be related to neurobiochemical disturbances which cluster in specific patterns. Understanding these patterns
will open the door for specific therapies based upon detoxification, reducing
oxidative stress and normalizing brain biochemistry. Asking these different questions and thinking about the
brain and its relationship to function in a very different way may lead to the
development of these new effective therapies. The practitioner of functional
medicine identifies the molecular uniqueness of the individual and then
intervenes with a specific therapy to help normalize neuronal biochemistry in
that unique individual. These emerging technologies, newly published research
studies and fearlessness on the part of clinician/researchers like Dr. Hoffer,
who demonstrate a willingness to open their minds to these new opportunities,
are paving the way toward the more effective management of neurochemical
disorders that have traditionally been outside the scope of successful
therapy. References 1. Hoffer A. Orthomolecular Medicine for
Physicians. Keats Publishing, New Canaan CT. 1989. 2. Hoffer A. Common Questions on
Schizophrenia and Their Answers. Keats Publishing, New Canaan CT.
1989. 3. Galland L. "Patient-Centered Diagnosis: A
Guide to the Rational Treatment of Patients as Individuals." Paper presented at
Second International Symposium on Functional Medicine, Rancho Mirage,
California, March 1994. 4. McHorney CA. "The Validity and Relative
Precisions of MOS Short- and Long-Form Health Status Scales and Dartmouth COOP
Charts: Results from the Medical Outcomes Study," Medical Care. Vol.30,
no.5.pp.MS253-65, 1992. 5. Anderson KE, Kappas A. "Dietary Regulation
of Cytochrome P450," Annual Review of Nutrition. Vol.11, pp. 141-67,
1991. 6. Caldwell J. "Conjugation Reactions in
Foreign-Compound Metabolism: Definition, Consequences, and Species Variations,"
Drug Metabolism Reviews. Vol. 13, no.5, pp.745-77, 1982. 7. Bland JS,BralleyJA. "Nutritional
Upregulation of Hepatic Detoxication Enzymes," Journal of Applied Nutrition.
Vol.44, nos.3&4, 1992. 8. Nolan JP. "Intestinal Endotoxins as
Mediators of Hepatic Injury An Idea Whose Time Has Come Again," Hepatology.
Vol.10, no.5, pp.887-91, 1989. 9. Klotz N,Ulrich N. "'Natural'
Benzodiazepines in Man," The Lancet. Vol.335, p.992, Apr. 14, 1990.
lO.Milbury PE, Doman G, Bland JS, Matson WR. "Oxidative Stress in Chronically
Brain Injured Children Evidenced by Metabolic Pattern Analysis." Submitted for
publication, 1994. 11. Bjarnason I, Williams P, So A, et al. "Intestinal
Permeability and Inflammation in Rheumatoid Arthritis: Effects of Non-Steroidal
Anti-Inflammatory Drugs," The Lancet. Pp. 1171-74, Nov.24,
1984. 12. Sherlock S. Diseases of the Liver and Biliary
System. Blackwell Scientific Publications, Boston, Mass., 1981. 13.Halliwell B, Gutteridge JMC. Free Radicals in Biology
and Medicine. Oxford University Press, New York, NY, 1991. 14. Staal F., Ela, S. Roederer M, et al. "Glutathione
Deficiency and Human Immunodeficiency Virus (HIV) Infection," The Lancet.
Vol.339, no.8798, pp.909-12, 1990. 15.0'Carroll RE, Hayes PC, Ebmeier KP, et al. "Regional
Cerebral Blood Flow and Cognitive Function in Patients with Chronic Liver
Disease "The Lancet. Vol.337, pp.1250-53, 1991. 16.Bakker HD, Scholte HR, Jeneson JA. "Vitamin E in a
Mitochondrial Myopathy with Proliferating Mitochondria," The Lancet.
Vol.342, no.8864, pp. 1175-76, 1993. 17. Mullen KD. "Benzodiazepine Compounds and Hepatic
Encephalopathy," New England Journal of Medicine. Vol.325, no.7,
pp.509-10, 1991. 18.Mullen KD. "Benzodiazepine Compounds and Hepatic
Encephalopathy," (editorial) New England Journal of Medicine. Vol.325,
no.7, pp/ 509-10, 1991. 19.Rothstein JD, Guidotti A, Tinuper P. "Endogenous
Benzodiazepine Receptor Ligands in Idiopathic Recurring Stupor," The Lancet.
Vol.340, pp. 1002-04, 1992. 20. Parker WD, Parks J, Filley CM, Kleinschmidt-DeMasters
BK. "Electron Transport Chain Defects in Alzheimer's Disease Brain,"
Neurology. Vol.44, pp. 1090-96. 21.Tetrud JW, Langston JW, Irwin I, Snow B. "Parkinsonism
Caused by Petroleum Waste Ingestion," Neurology. Vol.44,
pp.1051-54. 22. Steventon GB, Heafield MTE, Waring RH, et al.
"Xenobiotic Metabolism in Parkinson's Disease," Neurology. Vol.39,
pp.883-87, 1989. 23.Steventon GB, Heafield MTE, Sturman S, et al.
"Xenobiotic Metabolism in Alzheimer's Disease," Neurology. Vol.40, pp.
1095-98, 1990. 24.Fahn S. "The Endogenous Toxin Hypothesis of the Etiology
of Parkinson's Disease and a Pilot Trial of High-Dosage Antioxidants in an
Attempt to Slow the Progression of the Illness," Biochemistry and Health
Implications. The New York Academy Press, 1989. 25. Steventon GB, Williams AC, Waring RH, Pall HS.
"Xenobiotic Metabolism in Motoneuron Disease," The Lancet. Pp.644-47,
Sept 17, 1988. |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)