This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included.
FOR IMMEDIATE RELEASE
Orthomolecular Medicine News Service, January 26, 2022
Vitamin C and Infants
Determining dose
by Helen Saul Case
OMNS (Jan. 26, 2022) I am often asked about the vitamin C dosages that I gave my children when they were very little. I have not written an article specifically addressing how I got vitamin C into them when they were infants. This article is meant to fill that gap.
Daily Doses of Vitamin C
The day our children were born, we started supplementing with 50 milligrams (mg) per day of oral vitamin C. By age one, they were taking 1,000 mg of vitamin C per day in divided doses. These oral doses were in addition to the vitamin C they received through my breastmilk. (I was taking at least 8,000-10,000 mg of vitamin C per day while I was pregnant and while nursing.) We based these dosages on board certified chest physician Dr. Frederick R. Klenner's recommendation for infants of 50 mg per day. For healthy children, Frederick R. Klenner, MD, recommended 1,000 mg per day per year of age, leveling off at 10,000 mg per day when the child reaches ten years of age.
[1] This is when they were in GOOD health.
During their first year of life, we gradually moved up to Klenner's recommendation of 1,000 mg per day by age one. So as the months went by, we increased the dose. For example, at 6 months old, we gave them approximately 500 mg per day in divided doses. By age one, they were getting 1,000 mg per day.
Illness and High-dose C
When our infants were sick they received far more vitamin C per day. The amount of vitamin C depended on the child; it depended on the illness; it depended on the day. The goal was a happy, healthy baby. As my father Andrew W. Saul always says, "Take enough C to be symptom free, whatever the amount may be."
Practically speaking, we started our infants with a larger "loading dose" in the morning, then continued to give C throughout the day, every two hours or so. Once bowel tolerance (saturation) was reached, we cut back how much C we gave and how often we gave it, but we continued to give C regularly. If symptoms of sickness persisted, we did it again the next day, and the next. We wrote down the size of the dose and the time of day it was given. This helped us be consistent with dosing and helped us keep track of how much vitamin C was needed to get to bowel tolerance on a given day. We made sure they were eating well and were well hydrated.
"Every parent, and I mean everybody, wants to know exactly how much vitamin C their sick baby needs. The answer is, you need to determine this by experience on a case-by-case basis. That's what I did when the author of this article was four years old." (Andrew W. Saul)
Bowel tolerance is an indicator of oral dose vitamin C saturation. It is indicated by gas, a rumbling stomach, or slightly loose stool. If you take way too much C, very loose stool will result, but that goes away once doses are reduced.
[2] To determine bowel tolerance in infants, gassiness is a helpful early indicator of "enough" C. If bowel tolerance is reached and stools become frequent, liquid, or, as in the case of a breastfed baby, frequent and greenish in color (since they are always liquid-like), we know then to reduce the frequency and dose, but continue to give it regularly, ramping the frequency and dose up and down as the situation requires. This takes a little practice, but we know we're not hurting our children with extra C. It is a very, very safe vitamin.
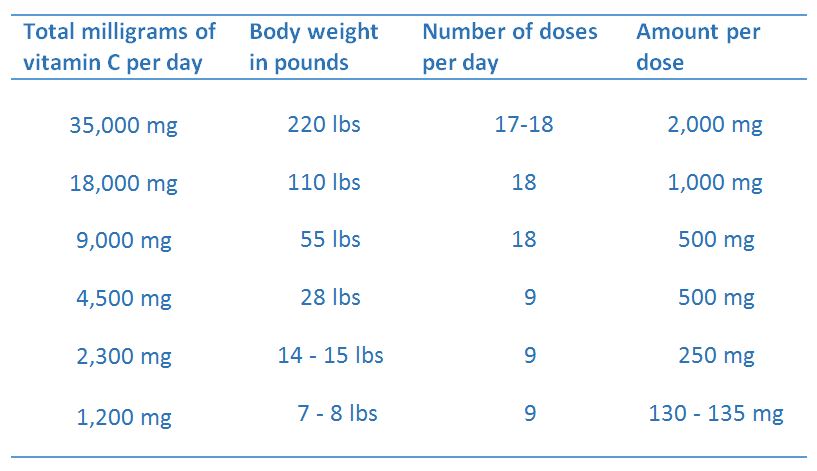
To help determine therapeutic doses of vitamin C for infants and growing children, I found this dosing table from Dr. Klenner helpful:
A Working Summary of Dr. Klenner's Formula: 350 mg Vitamin C per kg body weight per day
[3]
Infants and RSV
At six weeks old, my son was diagnosed by his pediatrician with RSV (respiratory syncytial virus) which caused cough and congestion. He had no fever, a good appetite, and while he was congested, he did not have trouble breathing. His oxygen level hovered around 92 or 93, and sometimes 94. (Even while the oxygen meter kept slipping off his tiny big toe.) The pediatrician wanted to see 95 or above. She recommended a bronchodilator drug. She said if the drug didn't help, oxygen and hospitalization were recommended. We were not comfortable giving an infant such a powerful drug, especially when we learned from Ralph Campbell, MD, that the drug was unlikely to help with the inflammation of the small branches of the bronchial tree, as seen in RSV. Additionally, the American Academy of Pediatrics said unless the oxygen reader was consistently below 90, supplemental oxygen would not be needed.
[4] Based on these facts, we decided to not give the drug and not to hospitalize our baby and would continue with home care. We made another appointment for the following morning for a pediatric checkup on his progress.
RSV can be serious. I wasn't about to take any chances. I got to saturation-level, bowel tolerance doses of vitamin C so that vitamin C would be available in my breastmilk. I also gave him liquid oral doses of vitamin C every two hours while symptoms persisted, and every three to four hours when they waned.
How did I know he was getting enough C? He got noticeably better: less congestion, no cough, alert, cheery and seemingly comfortable. When he and I had lots of C, his symptoms improved. As the C "wore off" at night when I was not taking C nor giving him oral doses, he would wake up with more prominent symptoms. His cough and congestion would return and he'd be fussy. I would then ramp of my intake of vitamin C and his. I would do this until he was visibly better, which would happen by the end of each day. By the end of the week, he was symptom free and back to his regular vitamin C intake. We avoided drugs. We avoided hospitalization. We gave high-dose C and watched it work.
Administering Vitamin C
While I was breastfeeding my infants, I took plenty of vitamin C to help ensure that it was available in my breastmilk. This was especially important when they were ill or before, during, and after vaccination. Personally speaking, the best way I got large doses of vitamin C into my infants was I myself took saturation level doses of vitamin C.
In addition to the vitamin C they were getting from my breastmilk, my infants could take vitamin C mixed into liquid by sucking it out of a dropper. Vitamin C can be added to baby's bottle of formula, but the form of vitamin C used matters. Specifically, sodium ascorbate vitamin C can be used because it is a buffered non-acidic form of vitamin C that won't curdle the milk.
Forms of Vitamin C
Our preferred form of vitamin C to give our children is sodium ascorbate vitamin C. This has come about after a great deal of experience using other forms of C. Sodium ascorbate vitamin C is easy on their stomachs and their taste buds, whereas ascorbic acid vitamin C is not. Sodium ascorbate just has a bit of a mild salty flavor, as its name suggests.
When my children were infants, I did not know about sodium ascorbate. At the time, I purchased a sweetened, prepared, children's liquid vitamin C. (I did not find a vitamin C liquid specific to infants.) It had a consistency that was a little thicker than orange juice, which made it easier for baby to drink out of a dropper. We would add extra vitamin C powder to the liquid C to increase the potency as needed, a mixture of about 80% ascorbic acid crystals buffered with 20% calcium ascorbate vitamin C powder. The liquid's sweetness helped mask the bitter taste of ascorbic acid. The liquid C contained a preservative, which normally I would avoid. However, the importance of having a delivery device for the vitamin C (one that baby would actually ingest) outweighed the presence of the preservative. Keeping C tasty is important, especially with children.
I would have much preferred to have known about (and used) sodium ascorbate vitamin C when my children were infants. A close family member mixes sodium ascorbate right into baby's formula bottle before each feeding, and the baby has always taken it without complaint. This is the method by which they give regular daily doses. This is also the method by which they get their baby to vitamin C saturation when warranted. (You would NOT want to mix ascorbic acid vitamin C into milk. It would taste awful.)
Daycare and School
The easiest way we got vitamin C into our children when they were away from home was to pre-mix the C into their food or beverages. For infants, sodium ascorbate C can be added to prepared bottles of milk. As they get older, vitamin C can be incorporated into yummy solid foods like applesauce. We are careful to give doses that are not too large so the child does not reach saturation while in the care of school or daycare personnel.
Vaccination
We gave saturation level vitamin C to our children for days before, the day of, and for days after every vaccination. I would get to saturation of vitamin C myself so lots of C was available in my breastmilk. I also gave them oral doses of vitamin C to bowel tolerance. I nursed them immediately after vaccination, right in the doctor's office. As they got older, I brought vitamin C dissolved in fruit juice and gave it to them right in the doctor's office. Vitamin C can also be mixed into formula or bottled breastmilk. We greatly prefer using sodium ascorbate for this purpose.
We have watched high-dose vitamin C safely prevent and treat vaccine side effects. We have watched high dose, saturation level vitamin C bring our 15-month-old daughter back to health after a severe vaccine reaction. We don't only give the amount of vitamin C we think might work; we give enough to get the job done.
Here are the articles I wrote about our experience:
- Our 15-month-old daughter's vaccine reaction and our use of high dose vitamin C: "Don't Vaccinate without Vitamin C" available at
http://www.orthomolecular.org/resources/omns/v11n09.shtml
- Answers questions about why we "chose" to get our children vaccinated: "Vaccinations, Vitamin C, and "Choice" available at
http://www.orthomolecular.org/resources/omns/v12n07.shtml
- Our five-year-old daughter's experience getting two MMR shots a month apart and the role of high-dose vitamin C: "Vitamin C Prevents Side Effects from the MMR Vaccine," available at
http://www.orthomolecular.org/resources/omns/v12n16.shtml When our younger son received the first of two MMR shots at age four, in addition to giving him saturation level, high-dose vitamin C before, during, and after his vaccination, we also followed the advice of pediatrician Ralph K. Campbell, MD, and gave him extra vitamin A. In addition to the beta-carotene present in his multivitamin and in the fresh, raw vegetable juice we give the kids each morning, he received 5,000 to 10,000 IU of oral supplemental preformed fish oil vitamin A the day before and the day of his MMR shot. We would administer the vitamin A by squeezing the contents of a gel tab onto a bit of yogurt. He, too, did not experience a single side effect due to the MMR vaccine.
Brands of Vitamin C
I don't endorse or recommend any vitamin brand. I do my very best to buy vitamins free of artificial sweeteners, artificial colors, and artificial flavors, and I call the company if I have questions about any ingredients or potency. I read and compare lots of labels and choose the best possible (and most affordable) option that gets results.
Disclaimer
I am not a doctor, and I believe you should work with yours. Diagnosis can be a valuable tool. I also know that if our children's pediatrician hands us a prescription for an antibiotic, antiviral, antihistamine, or antipyretic, most likely high-dose vitamin C can be used in place of any of them. But don't take my word for it. Look into vitamins and nutrition for yourself, and do what is best for you and your family. I believe we can be in charge of our own health and our children's health. Doing it ourselves does not mean it will be easy. It is an incredible amount of work to keep kids healthy. But it is worth it. As I've said before, sure, take your kids to their pediatrician. But wouldn't it be nice not to need to go?
(OMNS Assistant Editor Helen Saul Case is the author of The Vitamin Cure for Women's Health Problems; Vitamins & Pregnancy: The Real Story, and Orthomolecular Nutrition for Everyone.)
References
1. Klenner FR (1971) Observations on the dose and administration of ascorbic acid when employed beyond the range of a vitamin in human pathology. J Applied Nutrition 23: 61-87.
http://www.doctoryourself.com/klennerpaper.html
2. Cathcart RF (1981) Vitamin C, titrating to bowel tolerance, anascorbemia, and acute induced scurvy. Med Hypotheses. 7:1359-1376. Available at:
http://www.doctoryourself.com/titration.html
3. "Therapeutic Level of Vitamin C Supplementation as Employed by F. R. Klenner, MD" available at
http://www.doctoryourself.com/klenner_table.html
4. American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis (2006) Diagnosis and management of bronchiolitis. Pediatrics 118:1774-1793.
https://pubmed.ncbi.nlm.nih.gov/17015575
Further reading
Campbell R, Saul AW (2013) The Vitamin Cure for Infant and Toddler's Health Problems. Basic Health Publications. ISBN-13: 978-1591203032
Case HS (2016) Tips from a Megavitamin Mom: Getting Kids to Take Vitamins and Lots of Them. Orthomolecular Medicine News Service.
http://www.orthomolecular.org/resources/omns/v12n09.shtml
Case HS (2016) Vitamins & Pregnancy: The Real Story. Basic Health Publications (2016).
Case HS (2018) Vitamin C Questions: Answered. Orthomolecular Medicine News Service
http://www.orthomolecular.org/resources/omns/v14n12.shtml
Levy TE (2012) Vitamin C Prevents Vaccination Side Effects; Increases Effectiveness. Orthomolecular Medicine News Service.
http://orthomolecular.org/resources/omns/v08n07.shtml
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
Find a Doctor
To locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Albert G. B. Amoa, MB.Ch.B, Ph.D. (Ghana)
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Susan R. Downs, M.D., M.P.H. (USA)
Ron Ehrlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Claus Hancke, MD, FACAM (Denmark)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Dwight Kalita, Ph.D. (USA)
Felix I. D. Konotey-Ahulu, MD, FRCP, DTMH (Ghana)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Pedro Gonzalez Lombana, MD, MsC, PhD (Colombia)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Zhiyong Peng, M.D. (China)
Isabella Akyinbah Quakyi, Ph.D. (Ghana)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, M.D. (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, French Edition: Vladimir Arianoff, M.D. (Belgium)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Editor, Spanish Edition: Sonia Rita Rial, PhD (Argentina)
Contributing Editor: Thomas E. Levy, M.D., J.D. (USA)
Contributing Editor: Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Assistant Editor: Helen Saul Case, M.S. (USA)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Associate Technology Editor: Robert C. Kennedy, M.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
Comments and media contact: drsaul@doctoryourself.com OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication.
To Subscribe at no charge: http://www.orthomolecular.org/subscribe.html
To Unsubscribe from this list: http://www.orthomolecular.org/unsubscribe.html
|


