 |

|
|
|
|
 Back to 2000 4th Quarter Table of Contents
Back to 2000 4th Quarter Table of Contents
Introduction Ocular melanoma is characterized by a high rate of liver metastases. The median survival time is less than five months. There is no standard allopathic therapy for this condition.1 Although therapies based on the treat-ments of metastatic cutaneous melanoma have been tried, the conventional treatment of intravenous and intra-arterial hepatic infusions are usually futile. Systemic chemotherapies may cause temporary shrinkage of a tumor but will not cure the disease. Although the less toxic hepatic arterial infusion increases tumor shrinkage, there is no clear difference in survival rates between the two methods.2 Surgeons can resect isolated meta-stases, however this is not possible in the majority of cases either due to the tumor‘s size, multicentricity or adjacency to major blood vessels, or inadequacy of the hepatic functional reserve.3 Palliation is the stand-ard and sole treatment for most patients. Case and Treatment The following is a rare case of remis-sion of liver cancer through an initial treat-ment of chemotherapy followed by ortho-molecular treatment. The patient is a 76-year-old caucasian female with a history of ocular melanoma in the right eye treated with radiation implant. Three years after the radiation, a CT scan revealed multiple le-sions in the liver. The largest lesion was a 4.5 cm mass in the right lobe and at least three other lesions, 1-2 cm, throughout both lobes. A fine needle aspiration of the largest lesion confirmed the diagnosis of metastatic melanoma. Two months after the CT scan she began intrahepatic doxo-rubicin once 1. 124 Clay Street, Thomaston, CT 06787 each month for four consecutive months along with natural therapeutics. After the fourth month of treatment, chemotherapy was terminated and the patient received vitamin and botanical therapy exclusively. The CT scans indicated continuous regres-sion of liver tumor throughout the course of orthomolecular treatment for the next two years. Twenty-two months after the di-agnosis of liver cancer, the patient had no clinical evidence of recurrent liver disease, maintained body weight, appetite, and an active lifestyle. Patient 39 months later has no clinical signs of cancer. The basic natu-ral treatment consisted of the following min-erals, vitamins and botanicals: Vitamins\minerals: Taken daily in two di-vided doses. Vitamin C, 9 g Niacinamide, 500 mg Folic Acid, 15 mg Zinc, 100 mg Selenium, 100 mcg N-acetyl-cysteine, 1 g Botanicals: 45 ml of botanical combination tincture taken daily in two divided doses. Antineoplastic: Misteltoe, Chaparral Lymph drainage: Poke root, Cleavers, Bur-dock Immune Support: Astragalus, Echinacea Liver Support: Milk Thistle, Greater Cheladine. Adaptogens: Polygonium, Siberian Ginseng Digestive Support: Gentian The botanical dose prescribed is eight times the conventional dose typically used in North America. In natural medicine when treating serious cases, I feel it is im-perative to use high doses to treat condi-tions such as cancer. It is interesting to note that typically both patients and practitioners are often more afraid to use natural medicines in high doses than to use drugs in chemotherapy. Fear of natural healing processes has been ingrained in our mod-ern psyche along with comfort in taking toxic drugs. This fear prevents many peo-ple from gaining faith in taking such a pro-tocol. Fortunately, this patient had the commitment and faith to take both allo-pathic and natural medicine. To avoid habituation or side effects, different botanical combinations are cho-sen every three months. The above list con-tains the basic plants which I alternate. Usually one plant in each category is used for three months and then another one is substituted for the following three months. In addition, a daily massage of castor oil was applied topically over the liver to in-crease lymph drainage and to augment the white blood cell count.4 Three cups of or-ganic blueberries and rasberries were rec-ommended daily. With high levels of bioflavonoids, particular anthocyanins, these fruits provide excellent antioxidants.5 Rationale for Treatment The high dose of vitamin C at 9 g/day was used to enhance the immune system, stimulate collagen formation necessary for walling off tumors, inhibition of hyaluronadase which keeps the ground substance around the tumor intact and prevents metastases, prevention of onco-genic viruses, correction of an ascorbate deficiency, and reduction of of toxicity of doxorubicin.7 The use of Chaparral for cancer has been used traditionally by natives of the desert from Death Valley, the dry lands of Texas, the desolate mountains of the Sonoran, and the Mojave desert in Mexico. It is one of my favorite plants in the treat-ment of many conditions, among them cancer. Most Chaparral plants live for sev-eral hundred years, but some plants in the desert have been carbon-dated to be 11, 500 years old. A shrub that can live so long must have amazing medicinal properties. The plant has been shown to have over 600 me-dicinally active ingredients. Among them is NDGA (nordihydro-guaiaretic acid) a po-tent antioxidant.8 The efficacy of its anti-oxidant properties in preventing foods from becoming rancid was used not only by the indigenous Hispanics but also by modern Americans. Chaparral has been tradition-ally used for a variety of conditions rang-ing from melanoma to uterine fibroids. Al-though its anti-neoplastic activity is not understood by modern science, Chaparral has been used to treat melanoma with success. Perhaps part of its effect is its antioxidant and immune-stimulating activ-ity. There has, however, been documented cases of liver toxicity in people who have used Chaparral in extremely high dosages (i.e. 15 capsules daily for three months). Cases of known Chaparral poisoning favorably resolved when Chaparral was withdrawn. There have been no serious side effects in most people, even with high doses used in cancer, and no deaths reported.8 Milk Thistle contains the active con-stituent Silymarin, a mixture of flavono-lignans. Silibin, the most active flavolignan, is largely responsible for the benefits attrib-uted to the silymarin complex. Milk This-tle exerts a protective and restorative ef-fect on the liver. The hepatoprotective ef-fects include anti-oxidation, anti-lipid peroxidation, enhanced detoxification, and protection against glutathione depletion. Milk thistle inhibits the enzyme lipoxynase, thereby inhibiting the formation of the hepato-destructive leukotrienes. In dam-aged livers, silymarin has been shown to increase protein synthesis which might account for its hepato-restorative activity. Silymarin has been shown in animal stud-ies to possess anti-fibrotic activity, and anti-tumor activity in a range of cancers.9 Lymph health is imperative in a strong immune response. Poke root is a very pow-erful lymph drainer, however a small amount of no more than 10% of it should be used in a formula due to its potential toxicity. Fatal doses have been reported ingesting half an ounce of roots or berries in an adult. Siberian Ginseng is an excellent adaptogen and endocrine tonic. It has been shown to reduce leukopenia induced by endotoxins, prevent stress induced thymic and lymphatic involution, protect against ra-diation exposure, inhibit carcinogensis from urethane, 6 methylthiouracil, and indole.10 In all cancers absorption and digestion of nutrients is imperative. Considering that most cancer patients lose weight, any improvement in digestion is key. Gentian is a bitter herb that helps with appetite and the secretions of pan-creatic digestive enzymes. This patient was able to not only maintain body weight but have a 3.5 kg increase in weight throughout her can-cer treatment. She currently maintains an ac-tive lifestyle and feels well. Results Liver tumor size is now half and has re-gressed continously for the 33 months since chemotherapy was last administered. She currently has no hepatomegaly or elevated alkaline phosphotase which existed in the beginning of treatment. The following is a series of computed tomography reports throughout the pro-gression and remission of the patient’s metastatic melanoma. CT Scan Report, Month 1: Increased size and and number of hepatic lesions consistent with progression of hepatic metastatic disease. Multiple metastic foci, largest in posterior seg-ment of the right lobe measuring 4.5 cm. There are several lesions measuring 1-2 cm scattered in both the right and left lobe, superimposed on previous existing liver cysts. Biopsy indi-cates metastatic melanoma of the liver. Therapy Precribed: none Month 2: Multiple metastatic foci, larg-est in posterior of right lobe measring 4.5 cm. Increasing size and number of hepatic lesions compared to previous CT scan. Therapy prescribed: One dose of Intrahe-patic Doxorubicin, 90 mg/m2. Vitamin and botanical therapy. Month 3: Improvement in the meta-static disease in the right lobe of the liver. Therapy prescribed: One dose of Intrahe-patic Doxorubicin, 90 mg/m2. Vitamin and botanical therapy. Month 4: Improvement in the meta-static disease in the right lobe. Therapy prescribed: as previous Month 6: Large metastatic disease in the posterior of the right lobe of the liver has decreased slightly in size. Therapy pre-scribed: Vitamin and botanical therapy exclusively for the next 33 months. Month 8: Stable liver metastases and liver cysts. Month 11: No Change in liver metastases. Month 14: Improvement in the meta-static disease of the liver. Regression of the liver tumor. Month 20: Regression of liver tumor. Improvement in the metastatic disease of the liver. Month 21: Patient has no clinical evi-dence of recurrent liver disease. Further regression of liver tumor. Month 29: Patient has no clinical evi-dence of liver disease. Further regression of liver metastases. Month 39: Patient has no clinical evi-dence of liver disease. Further regression of liver metastases. The largest liver tumor decreased .5 cm from last CT scan. As Figure 1 (p.217) indicates, the nor-malization of alkaline phospotase demon-strates the reversal of liver disease. The continual decrease in the size of the liver tumors as evidenced by the CT scans indicated a remission of liver cancer. The largest tumor had decreased from 4 cm to 1.5 cm after 39 months of treatment. Although the oncologist thinks the pa-tient’s recovery was due to four days of chemotherapy administered three years ago, and that her naturopathic treatment has been only wasteful, I disagree. There is no evidence that chemotherapy in liver cancer has any possibility of causing remission especially years later. Currently there are no satisfactory allopathic treatment options for patients with ocular melanoma meta-static to the liver, and after liver metastases are identified, median survival time is only two to seven months.6 References
Figure 1. In 12 months consisting of 1 day of IV Doxorubicin and 12 months of vitamins and botanicals, serum values of alkaline phosphatase were within reference values and were maintained throughout the remaining treatment period. Normalization of Serum Values of Alkaline Phosphatase 350 300 250 200 150 100 50 0 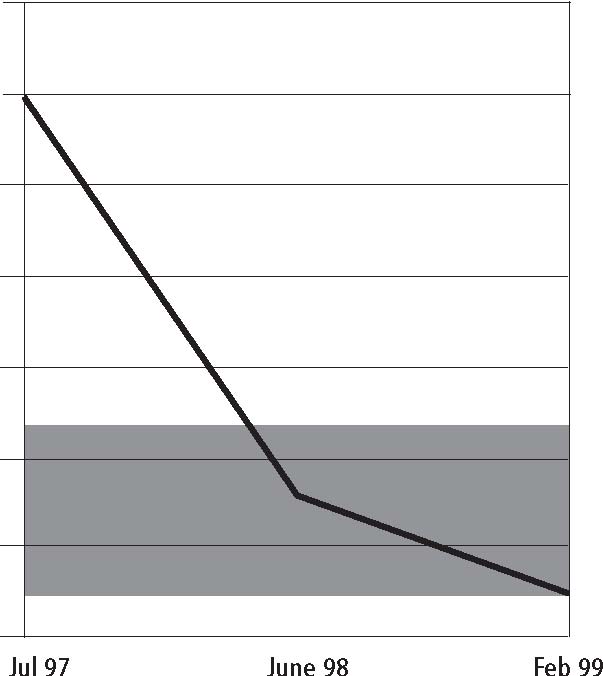 Alkaline Phosphatase |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)