 |

|
|
|
|
 Back to 1999 3rd Quarter Table of Contents
Back to 1999 3rd Quarter Table of Contents
Introduction The patient is a fifty-four-year old Caucasian female who has suffered from nineteen different pathologies. The magnitude of her serious health problems seemed almost impossible to reverse, but she was not an ordinary person. She had developed a remarkable inner strength and utmost determination to obtain emotional and physical health, something that she had never felt before. Her childhood was scarred with abuse: emotional, physical, and sexual. At the age of nineteen, she started to suffer from depression and was “treated” with eight electroconvulsive therapies. Since then, she has been hospitalized eight times for psychiatric episodes. At age forty-four, she was diagnosed with a personality disorder. At the age of fifty-three she became homeless. On our first visit in September, 1997, the chief medical concern was Diabetes Type 2, complicated by diseases that resulted from uncontrolled blood sugar levels. Diabanese, Metformin and Glyburide had been previously prescribed. However she had taken the medicine inconsistently for the last fifteen years, until May 1, 1997 when she completely refused all prescription drugs for diabetes. Five years after the initial diagnoses of diabetes twenty-five years ago, she developed the first signs of neuropathy with burning sensations running bilaterally in both hands and feet. At the age of forty-five, glaucoma and cataract formations were diagnosed. In the summer of 1997, kidney damage was diagnosed with microalbumin leaking out in micturation. Her health history included irritable bowel syndrome and colitis since birth. By her adolescence she had developed hy 1. 124 Clay Street, Thomaston, CT 06787 pothyroidism, toxemia, hypertension and tachycardia. In her twenties she developed diverticulitis. At age thirty she developed uterine hemorrhage due to a uterine fibroid. She also had uterine hyperplasia, an ovarian cyst and endometriosis. By her early forties a hysterectomy and cholecystectomy were performed. In May 1996, she was hospitalized with a blood pressure reading of 270/170 mm/Hg. Upon her first visit in September, 1997, the fasting blood sugar level was 22 mmol/L, and glycourea at 1 g/dL. The physical exam exhibited no patella or achilles reflex. There were pins-and-needle sensations and numbness running down the lateral sides of the legs. Treatment The patient refused all prescription drugs at this time to treat her blood sugar, due to the negative side effects of the drugs she had previously taken. To lower her blood sugar as quickly as possible, I prescribed an aggressive treatment including botanicals, mineral supplements and diet. The herbs were given in equal proportions. The dosage prescribed was 40 mL of tincture daily. Herbs were used to treat all organs that regulate blood sugar including the pancreas, liver and adrenal gland. Hypericum perforatum, a nervine, was used to restore nerve function. Solidago canadensis was used to help kidney function. Vaccinium myrtillus was prescribed not only as a hypoglycemic but also as a tonic for the eyes to treat the glaucoma. The herbs prescribed and the organs they treated are listed as follows: Liver Support: Silybum marianum Adrenal Support: Eleutherococcus senticosus Pancreatic Support: Jambolana syzigium, Oplopanax horridum Nervine Support: Hypericum perforatum Kidney Support: Solidago canadensis Eye Support: Vaccinium myrtillus Mineral supplementation included a multi-mineral formula that was specifically tailored to aid in blood sugar metabolism. This included a daily dose of 600 mcg chromium, 45 mg zinc, and 150 mcg selenium. Her diet was considered good in the conventional medical paradigm. However, this paradigm did not consider food allergens as a significant factor in the treatment of diabetes. She was very prone to food allergies due to her past history of digestive disorders and extreme dysbiosis. Studies have found that removing food sensitivities lower blood sugar levels dramatically.1 Thus a hypoallergenic diet was prescribed. Within three months of this diet she had consistent fully formed stools for the first time in her life. Results The following charts and tables demonstrate the effectiveness of the therapies prescribed. The treatment time was approximately one year. It took several months for the blood sugar to fall to 18mmol/L. The blood sugar consistently fell below 10 mmol/L after one year of treatment. These levels were below any level that she had achieved in the previous fifteen years, even with the daily use of Metformin 500mg b.i.d. and Glyburide 5 mg b.i.d. The effectiveness of St. John’s Wort in treating the neuropathy took about two months. When she discontinued this herb, the symptoms would come back, but with much less severity. The patient is now in much better emotional and physical health than she ever has been. In autumn 1999, she enrolled full time in a school to become a health care practitioner, and currently lectures on homelessness. References
Chart 1. Subjective assessment (as assessed by the patient).
Chart 2. Objective assessment (as assessed by lab tests). Before treatment After treatment Glaucoma 27mm/Hg 15 mm/Hg Fasting blood sugar 22.3 mmol/L 6.4 mmol/L Urine sugar 1 g/dL none Urine protein 500mg/dL 100-500 mg/dL Urine erythrocytes 250/uL 50-250/uL Microalbumin 3080 mmol/L 2775 mmol/L Glycosolated Hemoglobin .124 mmol/L .074 mmol/L Chart 3. Physical assessment of diabetic neuropathy an legs and hands. Before treatment After treatment Pins and needle sensation present not present numbness present not present burning sensations constant intermittent Case Report: The Use of Botanical and Mineral Supplementation to Treat NIDDM Figure 1. A halt in the natural progression of diabetic nephropathy,2 and a mild increase in kidney function as evidenced by a 10 percent decrease in urinary microalbumin secretion. Note: Reference level is 20 mmol/Hg. 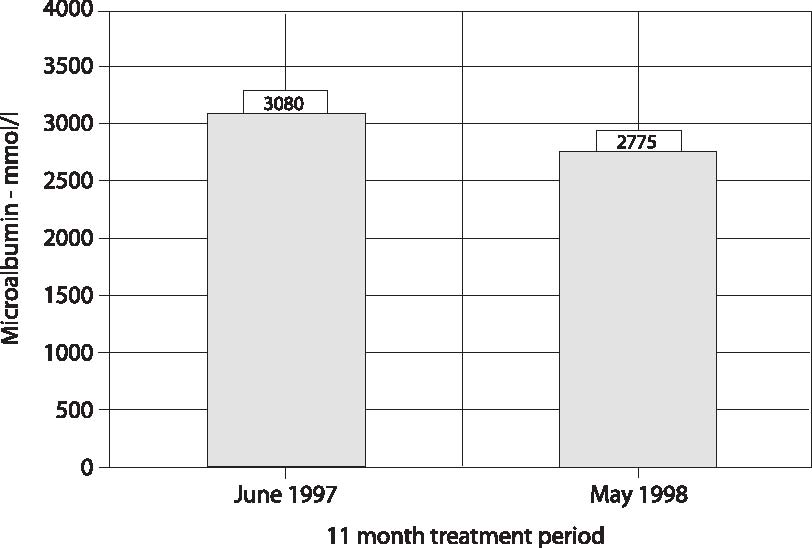 Figure 2. Reversal of secondary glaucoma as evidenced by a normal intra-ocular pressure. Note: Reference level for intraocular pressure is 15-20 mm/Hg. 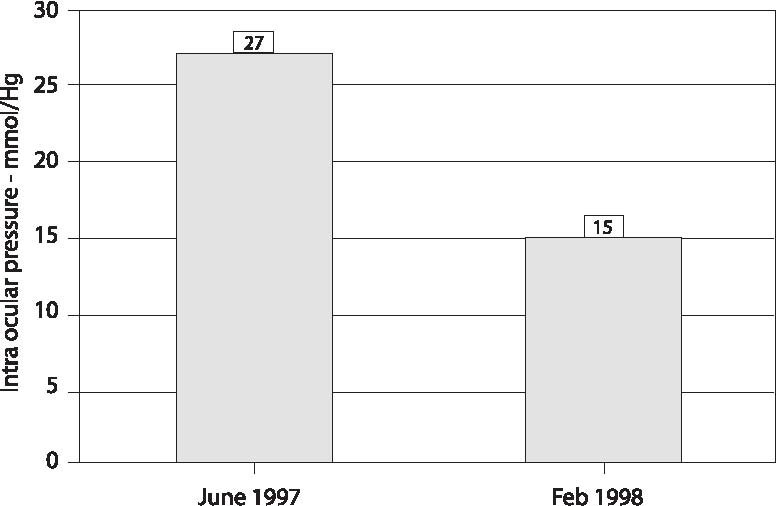 Diabetic glaucoma is due to a fibrovascular membrane growing over and sealing off the outflow channel of the eye. One can infer that a structural malformity has been reversed because the intra-ocuIar pressure level has been normalized. By decreasing glycosolation, denaturization of proteins is decreased, thus the formation of the fibrovascular membrane is inhibited. Along with the decrease of blood sugar and the antioxidant properties of Vaccinium myrtillus, the intra-ocular pressure has returned to normal. Journal of Orthomolecular Medicine Vol. 14, No. 3, 1999 Figure 3. A 44 percent decrease in glycosolated hemoglobin. The data shows that a marked long-term difference in total blood sugar has been achieved. Note: Reference levels .043 to .061 mmol/L.  11 month treatment period Figure 4. A 71 percent decline in fasting blood sugar. Fasting blood sugar level of 6.4 mmol/L in May, 1999, was the first normal blood sugar reading in 24 years. Results achieved without the use of Metformin and Glyburide. Note: Reference levels 3.6 to 6.4 mmol/L 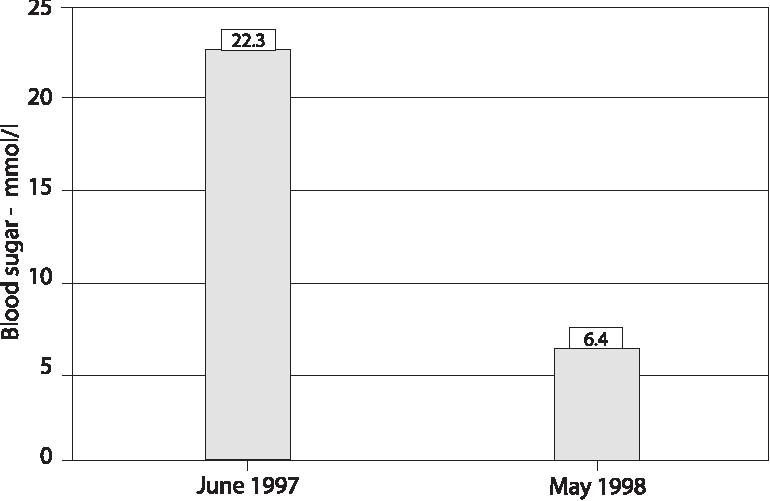 11 month treatment period | ||

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)