|

|
|
|
|
 Back to 1998 3rd Quarter Table of Contents
Back to 1998 3rd Quarter Table of Contents
Abstract This study looked at the relationship between myopia and mercury from dental fillings. Hair mercury levels were found to be significantly higher in 25 nonmyopic children compared to 25 myopic children. The researchers hypothesized that if mercury was leaching from the silver dental fillings, then subjects without dental fillings would have a higher degree of myopia and poorer acuity. A study comparing 51 subjects without amalgams to 50 subjects with amalgams confirmed this hypothesis. The non-amalgam group had a 59 percent higher degree of myopia and significantly poorer acuity. Two additional studies also found that subjects without amalgams had a higher degree of myopia. All three studies found that significantly more subjects without amalgams wore glasses for distance when compared to subjects with amalgams. The authors hypothesize that mercury may increase the collagen fibrils of the sclera and thereby retard the progression of myopia. Introduction Recent evidence suggests a relationship between mercury from dental fillings and adverse health.1,2 These studies show that subjects with silver dental fillings had significantly higher mercury levels in hair and urine when compared to subjects without silver fillings. The silver dental filling, commonly called the amalgam, is comprised of approximately 50 percent mercury.3 Studies have shown that mercury leaches from the amalgam in the form of elemental mercury vapor.4 and 74 to 80 percent of mercury vapor can be inhaled through the lungs to then enter l.Rocky Mountain Research Institute, Inc. 1304 South College Avenue Ft. Collins, CO 80524 Funded by a grant from The Wallace Genetic Foundation the bloodstream.5 Once it enters the bloodstream in the vaporized state, it can be transported to all parts of the body before it is ionized, and thus it can attach to various proteins.6 Mercury vapor also has an affinity for the eye.7 This paper reports on four phases of a study regarding the relationship between myopia and mercury from dental amalgam. Methods The first part of the study compared hair mercury levels in 25 children between the ages of 10 and 17 who had myopia to a control group of 25 age- and sex-matched subjects without myopia. Researchers cut a hair sample from the nape of each subject's neck and used atomic absorption spectrophotometry to analyze mercury levels. An eye refraction was also measured for all subjects. The second stage of the study compared the refractive status of 51 subjects without amalgams to a group of 50 subjects with amalgams. The nonamalgam group consisted of 30 females and 21 males who averaged 22.35 years in age. The amalgam group averaged 23.28 years in age and consisted of 30 females and 20 males. An ad was placed in the Colorado State University newspaper to solicit subjects. A refraction and unaided acuity at 20 feet was measured on all the subjects. A health questionnaire asked whether the subjects wore glasses for distance. A dental assistant charted the health status of each subject's mouth. The females averaged 9.8 amalgams, while the males averaged 10.1 amalgams. A similar study was then performed on a slightly younger age group with fewer fillings. The nonamalgam group averaged 19.25 years in age and consisted of 30 females and 23 males. The amalgam volunteers numbered 35 females and 20 males with a mean age of 19.28. The females had an average of 6.08 amalgams, and the males numbered 4.85. An eye refraction was conducted on all subjects with the examiner being blind to the status of the subjects. In the final stage of the research, the authors studied an older population of 25 females with an average of 13 amalgams. Their acuity and refraction were compared to a control group of 24 women without amalgams. The nonamalgam group averaged 34.45 years, and the amalgam group averaged 35.83 years. Again, the examiner remained blind to the status of the subjects. The Statistics Lab at Colorado State University performed statistical analysis. Analysis of variance and the student t test were performed on the numerical data. Statisticians used chi- squared for analysis of the questionnaires. A P (probability) level of 0.10 was considered significant for discussion purposes because of the low number of subjects and because the study was looking for trends. Results Phase I The subjects were grouped into categories reflecting sex, age, degree of myopia, and status of myopia. In 14 of the 25 myopes, both eyes measured a magnitude of over 2 diopters, and these subjects were categorized as the "higher" myopes. In the remaining 11 subjects, both eyes measured below 2 diopters of myopia and these subjects were distinguished as the "lower" myopes. Investigators used the spherical equivalent (adding the spherical myopia +1/2 the astigmatism) to determine the resultant power for category placement. The control group, referred to as the nonmyopes, consisted of 25 subjects whose spherical equivalent refraction was piano or in plus diopters. A category of "younger" myopes consisted of subjects aged 10 to 13, and "older" myopes consisted of subjects 14 to 17. The nonmyopes were categorized in these two age groups as well. Eleven male nonmyopes were compared to 12 male myopes, and 14 female nonmyopes were compared to 13 female myopes. Finally the general category of myopes was compared to nonmyopes. Hair mercury levels were significantly higher in nonmyopes than in myopes, in male nonmyopes than in male myopes, in younger nonmyopes than in younger myopes, and in older nonmyopes than in older myopes (Table 1, p.163). Phase II The mean refraction of the non-amalgam group was -2.42 diopters compared to -1.52 diopters in the amalgam group. This 59 percent difference was significant at the 0.028 level. Visual acuity averaged 20/205 in the nonamalgam group, and the amalgam group had a mean acuity of 20/122. This was significant at the 0.017 level. Thirty-four of the 48 nonamalgam subjects reported wearing glasses for distance, while 26 of 47 amalgam subjects said they wore glasses for distance. This 31 percent difference per group was significant at the 0.083 level (Table 2, p. 163). Phase III The 20 males with amalgams measured a mean refraction of -0.91 diopters of myopia, while the 23 males without averaged -1.12 diopters. This 23 percent difference per group was not statistically significant. The amalgam-bearing females averaged -1.63 D of myopia compared to -1.78 D in the nonamalgam subjects. The 9 per-cent difference per group was not statistically different. However, the health questionnaire found 15 of the 51 (29
percent) amalgam subjects wore glasses for distance, and 23 of 52 (44 percent)
nonamalgam volunteers reported wearing glasses for a distance correction. This
50 percent difference per group was significant at the 0.059
level (Table 3, p.163).
Table 1. Hair Mercury: Nonmyopes vs. Myopes Category Nonmyopes vs. Myopes vs. Lower Myopes vs. Higher
Myopes Mean ppm .141 .101 .018 .095 P Value .005 .047 .003 Standard Deviation .054 .035 .034 .035 Female Nonmyopes vs. Female Myopes .123 .100 .144 .044 .033 Male Nonmyopes vs. Male Myopes .166 .103 .010 .059 .039 Younger Nonmyopes vs. Younger Myopes .142 .099 .041 .053 .041 Older Nonmyopes vs. Older Myopes .140 .103 .065 .057 .030 Table 2. Questionnaire: Phase II Study Do you wear glasses for distance? Without Amalgams With Amalgams N = 48 N = 47 Yes No Yes No 34 12 26 21 % Difference = 31% P=0.083 Table 3. Questionnaire: Phase III Study Do you wear glasses for distance? Without Amalgams With Amalgams N = 52 N = 51 Yes No Yes No 23 29 15 36 % Difference = 50% P=0.059 Phase IV The group of older women (mean age = 35.83) with amalgams
had a mean refractive error of -1.94 diopters, while the women without amalgams
(mean age = 34.45) had a mean refraction of -2.44 diopters. The 26 percent
difference per group had a P level of 0.17. Acuities in the amalgam group
averaged 20/ 202 compared to 20/265 in the nonamalgam group (the P level was
0.18 [log 10]). The health questionnaire found that the women without
amalgams wore glasses more for distance (17 percent greater, P = 0.148) and near
(341 percent greater, P = 0.0008). (Table 4, below). Data Summary Of the total number of subjects who wore glasses, 78 of 124
(63 percent) without amalgams stated they wore glasses, and 58 of 123 (47
percent) volunteers with amalgams reported wearing glasses. This 34 percent
difference per group was significant at the 0.007 level. (Table 5, p.
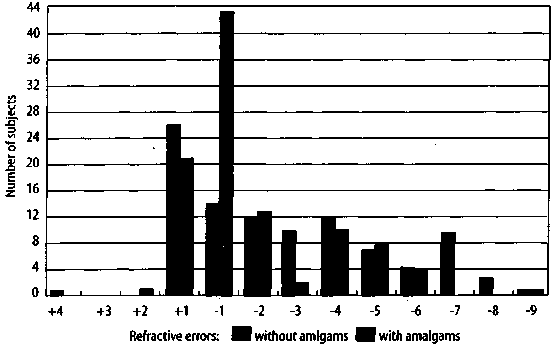
165) The refractive status of the two groups with an average of
ten amalgams (N=74) was then compared to the control group without amalgams
(N=75). Group members were age and sex matched. The nonamalgam group averaged
-2.43 diopters compared to -1.67 diopters in the amalgam group. This 46 percent
difference per group was significant at the 0.023 level. (Figure 1, p.
165) Discussion The study gives strong evidence that people without dental
amalgams have higher degrees of myopia when compared to a control group with
amalgams. Could mercury from dental amalgams be retarding the progression of
myopia? Mercury's involvement is further suggested by comparing the
hair mercury levels of children with myopia to those of children without myopia.
The children without myopia had significantly higher hair mercury levels,
indicating mercury may hinder myopias progression. This led to the hypothesis
that amalgam mercury may be one source of mercury. Studies have indicated that
people with dental amalgams have significantly higher mercury levels
in Table 4. Questionnaire: Phase IV Study Do you wear glasses for distance? Without Amalgams With Amalgams N = 26 N = 25 Yes No Yes No 21 5 17 8 % Difference = 17% P = 0.148 Do you wear glasses for near? Without Amalgams With Amalgams N = 26 N = 25 Yes No Yes No 14 12 3 22 % Difference = 341% P = 0.0008 Table 5. Summary of Questions Do you wear glasses for distance? Without Amalgams N = 124 Yes
No 78
46 % Difference = 34% chi squared 6.189 P = 0.007 With Amalgams N = 123 Yes
No 58
65 Figure 1. Comparision of refractive errors between subjects
with and without amalgams the brain,8 blood,9
urine,1 and hair.1 With this evidence, it was hypothesized
that subjects without amalgams would have higher levels of myopia. A study
comparing 51 nonamalgam subjects to 50 amalgam subjects, who averaged ten
amalgams confirmed this hypothesis. The nonamalgam group had myopia levels 59
percent higher than the amalgam group. The acuities in the nonamalgam group were
significantly worse as well. If mercury were involved, one would also expect a somewhat smaller difference in myopia in
subjects with fewer amalgams compared to a group with more amalgams. This was
confirmed in a study of college students whose average age was 19 years old,
with the amalgam group averaging approximately five amalgams. The males without
amalgams had myopia that averaged 23% higher, and the females without amalgams
had a 9% higher degree of myopia compared to the amalgam group. Though
measurement was not at the significant level, 50 percent more of the nonamalgam subjects reported wearing
glasses for distance. The last stage of the research confirmed that people
without amalgams had higher degrees of myopia. The women who averaged about 35
years in age and who averaged 13 amalgams and a mean degree of myopia that
averaged 26 percent higher than the amalgam group. If mercury does slow the progression of myopia, what is the
physiological mechanism? One cause of myopia is a disassocia-tion of scleral
collagen fiber cross-linking, which weakens the eyeball and results in
elongation of the eye.10 If mercury could increase the collagen
fibrils, perhaps this might retard the progression of myopia. Evidence indicates
that mercury can do this. A study by Roman-Franco et al.11 helps
support this hypothesis. They found that after mercuric chloride was
administered to rabbits, there was an increased amount of collagen fibrils in
the instituim around the tubular basement membrane of the kidney. Increased
amounts of collagen fibers also were found in the ileum and colon. Khayat et al.7 gave evidence that mercury does
have an affinity for the eye. They studied the distribution of inhaled
radioactive metallic mercury vapor (203 HgO) in rats and marmoset monkeys. The
microautoradio-gram found localized high concentrations in the retina
(especially in the receptor layer) and to a higher degree in the pigment
epithelium and choroid. Clinical evidence also suggests that mercury may play a
role in slowing the progression of myopia. During the 1950s C.
Desusclade,12 a French physician, used vitamin E and mercury to
retard the progression of myopia. He believed that myopic children may have a
deficient intake of dietary vitamin E, an exaggerated need for it, or trouble
assimilating vitamin E. His patients were instructed to take one or two 50-mg
tablets d-acetate d-alpha tocopherol (vitamin E) with water on an empty stomach
each morning for three months. After a several week discontinuance, a new series of daily doses
for three months was administered, and this regimen was followed at least once a
year. Rarely did myopia progress for children who followed this treatment. The
results improved when mercury was added to the diet. He believed vitamin E acts
on the fibril tissue of collagen. It is interesting to note that significantly more subjects
wore glasses for near vision in the group without amalgams. Several may have
been presbyopes. There were four subjects over 40 with amalgams who averaged 45
years of age compared to six subjects over 40 in the nonamalgam group who
averaged 45 years. However, one might assume that more subjects in the
nonamalgam group wore their glasses more frequently for reading if they had a
higher degree of myopia. Myopia and Dental Caries Several studies have investigated the relationship between
myopia and dental caries. Goldstein13 studied 87 men and 13 women
from the freshman class of the College of Medicine, State University of New
York. The study examined subjects to determine instances of caries in the four
lower premolar teeth. He chose premolars for examination because they were less
susceptible to caries. In the group having no caries in the four lower premolar
teeth, the study found the number of myopes no different from the number of
nonmyopes. Goldstein also found 17 subjects with four instances of caries; of
these, 15 were myopes and 2 were nonmyopes. When the number of low myopes was
compared to high myopes, there was no significant difference between the group
with four instances of caries and the group with no instances of caries. The
author concluded that because collagen is a significant component of dentin,
perhaps both myopia and dental caries are manifestations of a collagen
defect. Hirsch and Levin14 confirmed the find-ings of
Goldstein13 and found a positive relationship between myopia and the existence of dental
caries in the four premolar teeth. They also found a higher degree of myopia
among those persons with more caries in the four premolar teeth. Keller15
performed a study on 196 high school students to determine whether there
was a relationship between myopia and teeth that were decayed, missing, or
filled. He was not able to replicate the findings of Hirsch and
Levin14 or Goldstein.13 Keller concluded there was no
statistical relationship between myopia and dental caries. The
study15 did not report on the number of students who had no
caries. Summary This study consisted of four phases. The first phase
compared hair mercury in children without myopia to children with myopia. The
children without myopia had significantly higher levels of hair mercury. The
second phase of the study compared 51 subjects with a mean of ten amalgams to 50
subjects without amalgams, and the nonamalgam group had significantly higher
degrees of myopia and significantly poorer acuity. The next phase compared a
slightly younger population averaging approximately five amalgams to a sex- and
age-matched nonamalgam group. The nonamalgam group had higher degrees of myopia
but not at a significant level. However, the nonamalgam group reported
significantly more often that they wore glasses for distance. The final phase of
the study compared 26 older women without amalgams to 25 with amalgams. The
nonamalgam volunteers had 26 percent higher amounts of myopia, and 17 percent
more subjects in the nonamalgam group reported wearing glasses for distance. The
total number of subjects without amalgams in the study was then compared to the
total number with amalgams regarding whether they wore glasses for distance, and
34 percent more subjects without amalgams wore glasses for distance. The two
groups who had an average of ten amalgams or more had a 46 percent lower
magnitude of myopia compared to the group without amalgams. These data suggested
that mercury may retard myopia, and it is hypothesized that mercury may increase
the cross linking of scleral collagen fibers to cause the
retardation. References 1. Siblerud RL: The relationship between
mercury from dental amalgam and health. Toxic Substance J, 1990; 10:
425-444. 2. Siblerud RL: The relationship between
mercury from dental amalgam and mental health. Am J of Psychotherapy,
1989; XLIII: 575-587. 3. Bauer JG, First HA: The toxicity of mercury
in dental amalgam. Calif Dental Assoc J, 1982; 10:47-61. 4. Vimy MI, Lorschneider FL: Serial
measurements of intraoral air mercury: Estimation of daily dose from dental
amalgam. / Dent Res, 1985; 64:1072-1075. 5. Hursh JB, Clarkson TW, Cherian MG, et al:
Clearance of mercury (Hg-197, Hg-203) vapor inhaled by human subjects. Arch
Environ Health, 1976; 31: 302-309. 6. Clarkson TW: The pharmacology of mercury
compounds. Ann Rev Pharmacol, 1972;
12,375,406. 7. Khayat A, Dencker L: Organ and cellular
distribution of inhaled metallic mercury in the rat and marmoset monkey.
Actapharmacol et Toxicol, 1984; 55:145-152. 8. Eggleston DW, Nylander M: Correlation of
dental amalgam with mercury in brain tissue. Res Ed, 1987; 58:
704-770. 9. Abraham JE, Svare CW, Frank CW: The effect
of dental amalgam restorations of blood mercury levels. J Dent Res, 1984;
63: 71-73. 10. Curtin B: Scleral changes in pathological myopia
Trans. Am Acad Ophthal Otolarg, 1957; 62:777-788. 11. Roman-Franco AA, Turiello M, Albini B, et al:
Anti-basement membrane antibodies and antigen-antibody complexes in rabbits
injected with mercuric chloride. Clin Immunol Immunopathol, 1978;
9:464-481. 12. Desusclade C: La myopia evaluative pathogenic et
traitment par vitamin E. Press Medicale (Paris), 1967; 67:
855-856. 13. Goldstein JH: Myopia and dental caries. J Am
Med Assoc, 1971; 218: 1572-1573. 14. Hirsch MJ, Levin JM: Myopia and dental caries.
Am J Optometry and Arch Am Acad Med Assoc, 1973; 218: 484-488. 15. Keller JT: Evaluation of the relationship between
myopia and dental caries. Am J Optometry Physiol Optics, 1978;
55:661-669.
|

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)