 |

|
|
|
|
 Back to 1998 2nd Quarter Table of Contents
Back to 1998 2nd Quarter Table of Contents
Introduction Hypertension is the most prevalent cardiovascular disease. Approximately 30 million Americans have been diagnosed with hypertension1 and over 58 million Americans appear to be affected.2 Within certain segments of the medical profession, blood pressure thresholds and definitions for hypertension vary. Often, a systolic/ diastolic blood pressure of 140/90 mm Hg is used as a “borderline” to identify the transition from an acceptable blood pressure level into the realms of hypertension.3 For adults, borderline hypertension has been defined as a systolic blood pressure range between 140 and 160 mmHg and/or a diastolic blood pressure range between 90 and 95 mmHg. Absolute hypertension occurs, once the 160/95 mmHg limits have been exceeded.2 Background The majority of people with hypertension have essential hypertension. In their case, the high blood pressure condition does not have an obvious cause.3,4 Cardiac rate and cardiac output increase in some individuals with hypertension, but not all. However, an increase in total vascular peripheral resistance is a common characteristic of hypertension. Experimental Procedure Systolic/diastolic blood pressure and pulse rate were obtained for a number of individuals over a three year period. One of the individuals was a 58 year old male diagnosed with essential hypertension. Initially, his average systolic/diastolic blood pressure was approximately 176/104 mm Hg with episodes exceeding 210/118 mm Hg during periods of stress. Peak-to-peak systolic/diastolic blood pressure variations throughout the day of 60/18 mm Hg were fairly common. An echocardiogram revealed hypertrophy of the left ventricle. Records indicate that this person had an untreated high blood pressure problem for almost 16 years. After recording blood pressure data for nine months, this individual accepted medication for his condition, initially involving a 5 mg/day dose of Vasotec™ and ultimately a 20 mg/day dose of Zestril™ (ACE inhibitors). After taking the initial Vasotec™ prescription for 8 days, his average blood pressure dropped to approximately 152/90 mm Hg with peak-to-peak variations decreasing to 30/10 mm Hg. Although further intervention was discussed, the hypertense individual would not accept an increase in ACE inhibitor dosage and would not accept any other form of medication (ß-blockers, calcium channel blockers or diuretics). This person preferred to try other means of blood pressure reduction through diet, stress control, exercise and nutritional supplementation. There is some controversy concerning blood pressure variability and the impact of various kinds of activities and stress on blood pressure data. Part of this three year study involved recording blood pressure variations that can occur with stress (job related and family), eating, exercise, leisure time activities, relaxation, and sexual activity for an individual who has hypertension. The blood pressure-pulse rate data for the 58 year old male with hypertension was compared with data obtained for a 48 year old female, who was in good health, and a 17 year old high school student who was in very good shape (actively engaged in swimming and bicycling). The systolic and diastolic blood pressures vs. pulse rate data for these individuals was plotted graphically to detect any nonlinearities in their cardiovascular characteristics and identify significant differences in the slopes of the individual blood pressure vs. pulse rate characteristics. From an orthomolecular medicine standpoint, the effect of various nutritional supplements (vitamins, minerals, soy products, herbs) on blood pressure and blood pressure variations is of significant interest. One very interesting feature concerning the various methods that lower blood pressure involves their combined (cumulative) affect. Information on the ability of the various methods to lower blood pressure in a coherent additive manner or a non-coherent additive manner is very important from a treatment expectations standpoint. Finally, one topic that must be addressed involves the mechanisms that might be associated with essential hypertension. This condition may have a variety of causes.4 However, conventional physiological and biochemical models have not been able to provide enough information to clearly define a cause for this disease. Hypertension problems are often attributed to some form of malfunction in the renal system. In some cases, aberrations in kidney function can produce inappropriate levels of renin secretion, higher levels of angiotenson II production and increased aldosterone secretion. Essential hypertension is often responsive to treatment with angiotension converting enzyme (ACE) inhibitors. If this is the case, one might ask; “Are there other medical paradigms that might be considered so that an “obvious cause”, associated with the renal system, can be provided for some cases of essential hypertension?” A possible link to one of the mechanisms of essential hypertension could be associated with Dr. Björn Nordenström’s theory of Biologically Closed Electric Circuits (BCEC) and his description of Vascular-Interstitial Closed Electric Circuits (VICC).5,6 Charge transport can occur over VICC pathways because blood vessels can function as relatively insulated cables providing a pathway for tissue fluids and moving charges to reach the capillaries.7 After years of careful experimentation and analysis, Dr. Nordenström developed a theory involving continuous energy circulation and a corresponding electric/magnetic/ electromagnetic field circulation in living systems. Field circulation is accompanied by the co-transport of charged species (ions and electrons) forming continuous electric currents in the human body. These currents are maintained within various BCEC pathways in the body involving blood, interstial fluid, blood vessels, tissue, organs and neuromuscular units. Dr. Nordenström realized that by augmenting various healing processes normally associated with BCEC systems in the human body, electrotherapeutic techniques could be developed to treat a variety of diseases including cancer, neuromuscular disorders and cardiovascular disease. Dr. Björn Nordenström essentially “closed the loop” with respect to electrical activity in living systems. He described a closed system of adaptive electrical circulatory systems that maintain and regulate various functions and promote healing processes.8 In his booklet, Hypertension Report,9 Dr. Julian Whitaker makes a statement, regarding the treatment of hypertension with diuretics, that blends quite well with Nordenström’s BCEC theory. In the booklet, he states: “Water alone is the best diuretic, so for goodness sake, do your best to increase daily water consumption. This approach increases urine production and replaces the need for medication. Water allows the body to function at maximum efficiency and supports the hydroelectric mineral salts that convey electrical currents throughout the body.” From the standpoint of “convey[ing] electrical currents throughout the body,” Nordenström has measured endogenous electrical potential differences and electric currents between tissues and vascular components of the stomach, vena cava, aorta and left/right ureters of an anesthetized pig.7 Current flow between organs was observed for potential differences below 10 mV. Potential differences between the ureters and veins were in the range of -106 mV to +112 mV with VICC current levels of 1 μA to 15 μA. Nordenström’s results indicate that VICC systems can respond to very small changes in energy state and they can be activated at very low electric potentials. Therefore, in the absence of any physical damage or biochemical aberrations, a hydroelectric imbalance in the renal system could activate a number of mechanisms that promote hypertension. For instance, changes in electric potential can produce electric field variations that can have an effect on the porosity of capillaries, the pH of various body fluids, the movement of electrolytes and immune response.5 Capillary porosity and electrolyte movement can be affected by changes in localized electric fields. Therefore, the filtration process provided by the glomerular capillaries of the kidney, along with mechanisms associated with various renal clearance rates, could be affected by the 10 mV to 100 mV variations in potentials that occur between organs and various components of the renal system. In this case, BCEC theory and the VICC model could be the basis of a new medical paradigm that will help to explain some of the causes and mechanisms associated with essential hypertension. Results: Blood Pressure/Pulse Rate Characteristics Systolic and diastolic blood pressure/ pulse rate characteristics for a 58 year old man with essential hypertension, a 48 year old woman and a 17 year old high school student are shown in Figure 1a and Figure 1b (p.77). Several things stand out in these figures. The systolic characteristic (curve (a)) for the individual with hypertension shows a pronounced nonlinearity. The systolic characteristics for the other two non-hypertensive individuals (curve (b)) are on the same line. A portion of curve (a) and all of curve (b) intersect at a systolic blood pressure of approximately 214.5 mm Hg at zero pulse rate. A mathematical equation involving systolic blood pressure (BPs), pulse rate (PR), slope (ΔBPs/ΔPR) and standard deviation (σs) can be derived from the data used to produce Figure 1 (a): BPs = 214.5 mm Hg +(ΔBPs/ΔPR)(PR) ±σs. (1) For the systolic blood pressure curves of Figure 1a ΔBPs/ΔPR is approximately 0.96 mm Hg/beats per min. and σs is approximately 9 mm Hg for the hypertensive individual and approximately 1.43 mm Hg/ beats per min. and 5 mm Hg for the non-hypertensive individuals. The higher systolic blood pressure levels for the hypertensive individual are most likely due to variations in cardiac output. The lower slope (ΔBPs/ΔPR) for the lower portion of the hypertense individual’s blood pressure characteristics would tend to indicate that it is more difficult to promote increases in cardiac output (cardiac rate X blood volume) as average blood pressure increases. In this case, the arterial capacitance (Ca, where Ca = ΔVolume/ΔPressure) decreases at the higher blood pressure levels because of limitations on volume increases and elasticity with increased blood pressure. The sharp increase in slope for the upper portion of the curve could be indicative of an abnormality associated with increase in arterial impedance. The arterial impedance increase at the higher blood pressure levels could be due to the combination of a reduction in arterial capacitance (which relates to elasticity) and an increase in resistance due to stress and turbulent blood flow. Certain forms of turbulence can be produced by large surges of Figure 1a: Systolic blood pressure vs. heart rate for an individual with hypertension (curve a) and two non-hypertensive individuals (curve b). One of the nonhypertensive individuals is a well conditioned 17 year old athlete. His blood pressure-heart rate data are in the upper end of curve b, where the heart rate is lower and the blood pressure is higher. The lower end of curve b involves the blood pressure-heart rate data for a 48 year old woman who is in good health. Her blood pressure is typically lower and heart rate is higher compared with the 17 year old athlete. 220
Figure 1b: Diastolic blood pressure vs. heart rate for an individual with hypertension (curve a) and two non-hypertensive individuals (curve b). 120 100 80 60 40 20 0
ejected blood from the hypertensive individual’s enlarged left ventricle. In addition, this nonlinear characteristic indicates that for larger and larger increments of heart rate, the incremental change in systolic blood pressure tends to decrease. This could be indicative of the arterial capacitance variations that promote orthostatic intolerance conditions sometimes associated with reno-vascular hypertension and essential hypertension.10 In Figure 1b, curve (a) and curve (b) intersect at a pulse rate of approximately 140 beats per minute at zero diastolic blood pressure. A mathematical equation involving diastolic blood pressure (BPd), pulse rate (PR), slope (ΔBPd/ΔPR) and standard deviation (σd) can be derived from the data used to produce Figure 1b. BPd = (ΔBPd/ΔPR)(140 beats per min.-PR) ±σd (2) For the diastolic blood pressure curves of Figure 1b, ΔBPd/ΔPR and σd are approximately 1.2 mm Hg/beats per min. and 9 mm Hg for the hypertensive individual and approximately 0.9 mm Hg/beats per min. and 4 mm Hg for the non-hypertensive individuals. Slope comparisons associated with the diastolic characteristics (ΔBPd/ΔPR) of Figure 1b indicate a higher vascular peripheral resistance for the hypertensive individual. The hypertensive individual’s hypertrophy condition has resulted in a thicker left ventricle wall, and a reduced left ventricular chamber volume. This condition, defined as concentric left ventricle hypertrophy is most closely associated with hypertension and is accompanied by an increase in total peripheral resistance.11 Generally, a rise in total peripheral resistance increases the diastolic blood pressure more than it increases the systolic. Increases in cardiac output generally raise the systolic blood pressure more than the diastolic.3 For situations where the hypertense individual’s blood pressure is increasing, the higher slope at high systolic blood pressures could be indicative of a higher peripheral resistance along with a higher cardiac output (cardiac rate). This resistance increase could be due a number of interactive mechanisms including the effects of turbulent blood flow. As previously mentioned, turbulence can occur as a large volume of blood is forced out of the left ventricle chamber by the enhanced contractions from a thicker left ventricle wall. At lower blood pressures, the left ventricle contractions would not be as forceful. This could contribute to significant reductions in cardiac output and a reduction in turbulent blood flow. The reduced turbulence would promote a more smooth laminar blood flow and contribute to a lower peripheral resistance. Blood Pressure Reduction Approach: Base-line Conditions and Initial Therapeutic Approach Blood pressure data was recorded daily for this person over a three year time frame. Very pronounced cyclical variations were measured on a daily, weekly and monthly basis, and a six month cycle was also noticeable. The average (baseline) blood pressure for the hypertensive individual was approximately 170/103 mm Hg with very large blood pressure peak variations. After a full meal, this individual could suffer incremental blood pressure increases up to 45/20 mm Hg. In addition, incidences of family and work related stress caused incremental blood pressure increases up to 40/15 mm Hg. At times, blood pressure readings of 210/118 mm Hg were observed at home, work and at the doctor’s office. During periods of reduced work, summer vacations and work breaks; a consistent decrease in incremental blood pressure was recorded. From this data, it appears that the work environment contributes approximately 15/9 mm Hg to this individual’s hypertension problem. However, from the baseline data, it would appear that the work environment is not the primary cause of this person’s high blood pressure problems. As a first therapeutic step, the hypertense individual agreed to take an ACE inhibitor (5 mg Vasotec™ initially, eventually progressing to 25 mg of Zestril™). He would not consent to taking any ß-blockers, Calcium channel blockers or diuretics for his hypertension problem. His average blood pressure decreased to 150/90 mm Hg, with significantly lower blood pressure variations. Initially, some adverse effects were noted (diarrhea and fatigue), and these symptoms subsided after a week on the medication. Increasing the prescription by 50% produced an additional reduction in systolic blood pressure of approximately 7 mm Hg. However, the increased intake of the drug caused a significant increase in fatigue along with coordination problems, dizzy spells and depression. At this point, it was clear that the primary approach toward blood pressure control could have its share of health hazards if it was based on drug therapy alone. Blood Pressure Reduction: From an Orthomolecular Medicine Approach The initial approach toward blood pressure control involved diet. A lower intake of fat and processed sugar produced a blood pressure incremental decrease of 15/ 6 mm Hg over a period of three weeks. However, blood pressure variations remained high. One of the simplest and most effective therapeutic approaches involved the combination of a significantly higher water intake, and supplementation with lecithin (3600 mg/day) and L-carnitine (500 mg/ day). Increasing water intake can help to promote a better hydroelectric and sodium-potassium balance in the renal system. Lecithin (phosphatidyl choline) will promote the synthesis of acetylcholine, a neurotransmitter that tends to reduce blood pressure. L-carnitine is important in the oxidation of fatty acids and is sometimes described as an oral chelating agent. As Figure 2 (p.101) indicates, the combination of these three substances promoted an incremental blood pressure reduction of 16/8 mm Hg over a period of twelve days. One of the interesting characteristics associated with this approach involves a three day lag before any noticeable response is observed. The hypertense individual also noticed that the nocturnal reduction in systolic and diastolic blood pressure began to return. Prior to this, his blood pressure was often higher in the morning than it was the evening before. In addition, previous to this, systolic blood pressure incremental increases were often quite high (≥ 45 mm Hg) after eating a full meal. After the water/lecithin/L-carnitine combination was implemented, incremental increases in systolic blood pressure were significantly lower (≤25 mm Hg) after eating a full meal. In many cases, exercise and weight lifting (in moderation) are recommended for blood pressure control. This particular hypertense individual tried a number of exercise programs and found them to be beneficial in a number of areas (including energy and ability to sleep), but very little reduction in blood pressure was observed with exercise. In fact, often, when he was exercising the most, these were the time periods when his average blood pressure readings were at their higher levels. A soy product called raffinee-a produced a response similar to the one observed with the water/lecithin/L-carnitine combination. Taking two vials per day of this nutritional supplement produced a 12/7 mm Hg incremental decrease in blood pressure (Figure 3, p.102). What is interesting about this nutritional supplement is that no response was observed for approximately 3 days. Several other individuals, who were not taking medication for hypertension saw significant reductions in blood pressure. In one instance, a 64 year old male recorded a decrease in blood pressure from Figure 2. Blood pressure reduction as a result of an increase in water intake and a daily nutritional supplementation of 3600 mg of lecithin and 500 mg of L-carnitine. Notice that as systolic blood pressure increases, often, the diastolic blood pressure decreases for the hypertensive individual. 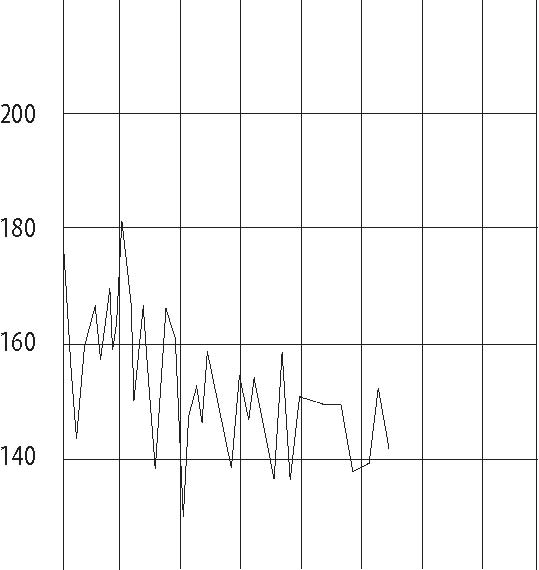 02 4 6 8101214 Day 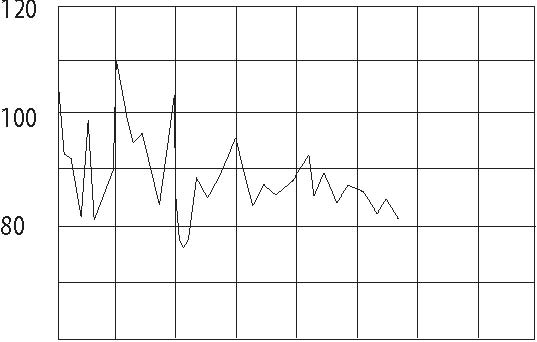 02 4 6 8101214 Day 140/90 mm Hg to 120/70 mm Hg taking (20,000 IU/day), Ca/Mg (600/300 mg/day), three vials of raffinee-a each day. vitamin B complex, niacin (300 mg/day), A variety of supplements were taken flaxseed oil 500 mg/day), coenzyme Q10 in order to promote cardiovascular condi-(60 mg/day), zinc picolinate (30 mg/day), tioning and reduce blood pressure. These ginko biloba (100 mg/day), bilberry ex-supplements included beta carotene tract (250 mg/day), horse chestnut extract Figure 3. Blood pressure reduction measured with the nutritional supplement raffinee-a (a soy product) for the hypertensive individual. Again, notice that when systolic blood pressure increases, in some cases, the diastolic blood pressure decreases. 200 180 160 140 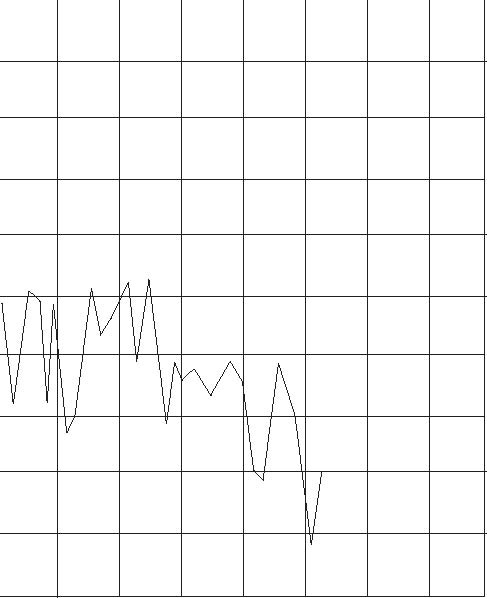 02 4 6 8101214 Day 120 100 80 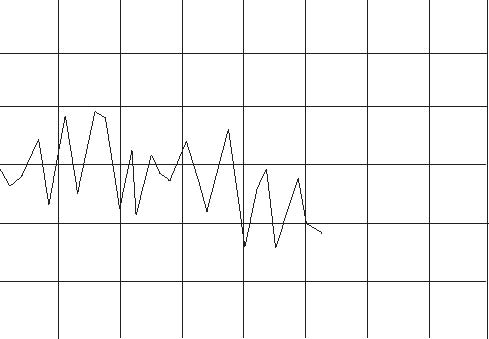 02 468 (400 mg/day) and potassium (100 mg/ day). The most pronounced effect observed with this combination was a 10 mm Hg reduction in diastolic blood pressure (indicating a reduction in total peripheral resistance). There was no significant reduction in systolic blood pressure (indicating a minimal effect on cardiac rate or 1012 14 Day blood volume). Also, no additional decrease in diastolic blood pressure was observed for this individual when these supplements were increased. Another factor in blood pressure control involves the reduction of cholesterol and triglycerides. A number of nutritional supplements were taken each day by the individual with hypertension in an attempt to reduce his total cholesterol level (223 mg/dL) and triglyceride level (208 mg/dL). The list of supplements included cayenne pepper (40,000 HU), Ω3 fish oil (500 mg), vitamin C (1000 mg), L-carnitine (500 mg), pycnogenol (100 mg), vitamin E (800 IU), L-lysine (500 mg), garlic (400 mg), selenium (200 mcg), inositol (150 mg), licorice root and L-arginine (100 mg). Within a year, his cholesterol level decreased to 177 mg/dL and his triglyceride level decreased to 131 mg/dL. The cholesterol and triglyceride reduction did not seem to produce significant reductions in average blood pressure levels. However, some reduction in day-to-day incremental blood pressure variations was observed over that time frame. In the analysis of the various items that increase and decrease blood pressure; the three year study strongly indicates that one must be very careful not to utilize coherent addition in the analytical approach. For instance, assume a certain supplemental herb, by itself, reduces systolic blood pressure by 10 mm Hg. Assume another nutritional supplement, by itself, also reduces systolic blood pressure by 10 mm Hg. When the two supplements are combined, the total reduction in systolic blood pressure will not be 20 mm Hg. In this case, the process of non-coherent addition is more applicable. When the two supplements are combined, the total reduction in systolic blood pressure will be closer to 14 mm Hg, ie. ((102 +102)H mm Hg= 14.14 mm Hg). Combining substances that reduce blood pressure does produce a cumulative effect. However, under the constraints of non-coherent addition, the substances that have the smaller effects do not accumulate as efficiently as one would expect when they are combined with substances that produce more pronounced reductions in blood pressure. Conclusions Blood pressure reduction for individuals with hypertension is strategically important not only for cardiovascular health, but also from the standpoint of minimizing kidney damage. However, blood pressure medications appear to have their own complications and dangers. Certain diuretics can deplete potassium and magnesium levels and increase cholesterol and triglyceride levels. They can cause digestive stress, muscle spasms, problems with renal dysfunction and aplastic anemia along with increasing the risk of heart attack and cardiac arrhythmias.12,13 Beta-blockers can promote impotence, fatigue, depression and congestive heart failure in susceptible patients.12,14 Calcium channel blockers can weaken the heart and damage the liver.12,14 Adverse consequences associated with ACE inhibitors are generally not quite as severe as those associated with other medications. In fact some improvement with insulin sensitivity in patients with insulin resistance and some cholesterol reduction may occur in patients with certain renal diseases.14 However, the attempt to go off the ACE inhibitor can produce a very significant rebound effect. In this case, the blood pressure goes to a higher level than it was previously. Clearly, alternative forms of blood pressure control are desirable, especially from a long-term standpoint. Often, diet and control of the work environment will be recommended as primary therapeutic approaches toward the treatment of high blood pressure. The results of this three year study on hypertension indicate that focusing on a recommendation like this may not be the best approach for some people afflicted with hypertension. In most cases, blood pressure problems have underlying physiological reasons, and the physiological deficiencies must be corrected. For older people, there are usually a large number of interactive deficiencies that must be addressed. The hypertense individual in this 3 year study has a number of inter-related health problems that are contributing to his high blood pressure condition. First of all, based on his responses, he is obviously dehydrated. This is a very common problem in many older people and is often the root cause for a variety of health problems ranging from cardiovascular disease to lower back pain.9 Referring to Whitaker’s statement and Nordenström’s BCEC/VICC model of the renal/vascular system, deficiencies in the body’s hydroelectric system can promote aberrations in the electric potentials between various VICC components (ureters, blood vessels, other organs). Small variations in these potentials can have a significant influence in filtration processes, electrolyte balance and renal clearance rates. This model appears to be appropriate for the essential hypertension condition, and it would appear that, for many individuals, water intake is one of the first primary items to address for the treatment of essential hypertension. Electrical imbalances in the renal system could contribute to a hypertension problem that eventually damages the renal system, which will produce additional complications for the high blood pressure condition. Along with increased water intake, it would also appear that essential hypertension problems could be addressed by recommending a certain amount of lecithin and L-carnitine supplementation. L-carnitine is biosynthesized in the liver. Any decreased liver function, often associated with aging processes, could require supplementation of this amino acid. The second primary item to be addressed involves the high diastolic blood pressure levels. The cardiovascular system is under the influence of the diastolic pressure for most of the cardiac cycle. The total peripheral resistance is indicated by the diastolic pressure, and diastolic pressures of 104 mm Hg to 118 mm Hg are unacceptable. Nutritional supplementation included vitamin A, Ca/ Mg, vitamin B complex, niacin, flaxseed oil, coenzyme Q10, zinc picolinate, ginko biloba, bilberry extract, horse chestnut, potassium and raffinee-a would appear to be the next step in the therapeutic process to reduce total peripheral resistance and help to promote renal system electrolyte balance. The third item is partially addressed in the first two items. It involves long-term remediation of cholesterol and triglycerides contributing to overall cardiovascular health and the minimization of extremes in blood pressure incremental variations. Once cardiovascular and renal health problems have been addressed, appropriate, safe and realistic exercise and work environment control programs can be incorporated. Acknowledgements The author wishes to thank Professor Björn Nordenström and Carl Firley, President and North American Vice President of the International Association for Biologically Closed Electric Circuts in Biomedicine (IABC) for their helpful comments and suggestions. Additional discussions with Dr. Steve Mercurio, Department of Biological Sciences, Mankato State University, Mankato, MN and Michael B. Rath, MD, Mankato Clinic, Mankato, MN are also gratefully acknowledged. References
Publications, 1983.
|

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)