 |

|
|
|
|
 Back to 1998 1st Quarter Table of Contents
Back to 1998 1st Quarter Table of Contents
From Holland to Jamaica; from the 18th Century to 1988 In the 18th century, a midwife in Friesland, in the northern part of The Netherlands, kept meticulous records of her professional activities.1 Her name was Catherina Schrader. In the periods 1722- 23 and 1732-33 she reported a high amount of six births of babies with neural tube defects in 3100 babies1 (1.9:1000). Both periods seemed to correspond with unusually poor crops. The neural tube defects occurred mainly in babies of poor urban women, who likely had reduced access to good sources of nutrition. Now, on the basis of current knowledge of the relationship between the development of NTD and a poor periconceptional supply of folic acid, we can state that Shrader’s records may indicate a deficiency of this B vitamin. Interestingly, a similar phenomenon was seen in Jamaica in 1989/1990.2,3 Nine months after the hurricane Gilbert (September 12, 1988), the incidence of neural tube defects increased. Normally the NTD rate in Jamaica is 1.4 per 10,000 live births. After Gilbert, the mean incidence was 3.9, peaking at 5.7. Coincidentally there was a rise in megaloblastic change in sickle cell patients, which was due to folate deficiency.3 It was also suspected that the high NTD incidence was folate dependent, since after the hurricane the access to fruit and vegetables, rich in folic acid, was reduced, and these products were more expensive. Tip of the Iceberg These two useful stories are examples of the relationship between weather circumstances, the availability of folate-rich food, and the consequence of specific illnesses such as NTD and anemia. With 20th century research, it is possible to explain these relationships biochemically. Also, with understanding of these underlying biochemical mechanisms, the involvement of other nutrients and other illnesses can be demonstrated. The current scientifically proven and accepted folate deficiency as a risk factor for NTD,4 is only the tip of the iceberg. An historical review of this particular relationship reveals how difficult it is for such a concept to become generally accepted. A Brief Recent History In 1960 at the Ciba Foundation Symposium, M.M. Nelson reported congenital malformations in rat embryos as a consequence of folate deficiency. In 1965, the Scottish physicians Hibbard and Smithells reported a study in 98 women with NTD babies. They suggested that these malformations may be due to a defect in folate metabolism.5 In 1970, Baumschlag et al. published in the British Medical Journal a study in Bantues with a low folate intake in comparison with whites with adequate folate supply.6 These researchers recommended, on the basis of their findings, folate supplementation during pregnancy. In 1976 an examination of the blood of 900 pregnant women, showed that six mothers with NTD babies had significantly lower levels of folate and vitamin C.7 In 1980, Smithells et al. demonstrated that women, who previously had a child with NTD, were protected by a multivitamin supplement from any further occurrence of babies with NTD. The prevalence in the supplemented women was one NTD case in 178; in the non-supplemented group 13 cases of 260 babies.8 Laurence et al. stated in 1981 in the British Medical Journal: “It is concluded that folic acid supplementation might be a cheap, safe, and effective method of primary prevention of neural tube defects, but that this must be confirmed in a large, multicentre trial”.9 Smithells et al. conducted further studies; all the results pointed in the same direction.10,11 Vitamin supplementation, especially folic acid prevents the occurrence of NTD. Continued discussion, mainly dealing with the ethical question, whether it had been sufficiently proven that folic acid could prevent neural tube defects, occurred in The Lancet from 1980 until 1984. Eventually, it was decided to conduct a final multicentre study. The results were published in The Lancet in 1991, eight years later. Conclusion: “Folic acid supplementation starting before pregnancy can now be firmly recommended for all women who have had an affected pregnancy, and public health measures should be taken to ensure that the diet of all women who may bear children contains an adequate amount of folic acid.”4 This multicentre study is now regarded as the ultimate proof that adequate folate prevents neural tube defects. On the basis of this, in The Netherlands, as well in other European countries, public campaigns have begun to inform women who wish to become pregnant about the benefits of folate. These campaigns began in 1995, 35 years after the initial presumptions that there is a relationship between inadequate folic status and NTDs. Natural Food vs. Supplementation in the Medical Research Council Vitamin Study4 The authors mention that the diet should contain adequate amounts of folic acid. Cuskelly et al.12 investigated the effectiveness of the intake of folate with natural food, foods fortified with folic acid and supplements.12 The results show that it was impossible to elevate the red-cell folate concentrations sufficiently with natural food, in spite of aggressive intervention. The authors concluded: “We have shown that compared with supplements and fortified food, consumption of extra folate as natural food folate is relatively ineffective at increasing folate status. We believe that advice to women to consume folate-rich foods as a means to optimise folate status is misleading.” It is generally accepted now that the intake of folic acid should be at least 400 mcg per day. It is not possible to achieve this amount with normal eating habits. Other means, as food fortifying or food supplementation, are necessary to repair this shortcoming in the daily diet. This phenomenon can be regarded as a precedent in the history of nutritional science. Never before have healthy persons, in this case expectant mothers, been recommended to take supplements for preventive reasons. Moreover, it took almost 40 years to get the idea generally accepted. Pathophysiology The transfer of methyl groups (-CH3) is a vital aspect in human metabolism. If there are not enough methyl groups available, the synthesis of some substances with crucial functions may be inadequate. This may have clinical consequences. To these substances belong the nucleic acids, the building stones of DNA. One clinical consequence may be the insufficient development of the neural tube. Another consequence is the development of anemia. The availability of methyl groups is dependent on adequate methylation functioning, as shown in Figure 1, (p. 54). There must be sufficient concentrations of S-adenosylmethionine, which is formed from methionine. Methionine is synthetized when sufficient amounts of 5-methyl-tetrahydrofolate and methylco-balamin are available. These two substances are the active forms, respectively, of folic acid and vitamin B12. When levels of folate and B12 are inadequate, there is poor availability of methyl groups, and an increased level of homocysteine. Figure 1. A) Methylation: Methyl groups (-CH3), available via the conversion of S-adenosylmethionine to S-adenosylhomocysteine, are necessary for the synthesis of nucleic acids and neurotransmitters. Under normal circumstances, homocysteine will be converted into methionine with the assistance of the active forms of folate and vitamin B12. B) Transsulfuration: Via the transsulfuration pathway, homocysteine is converted into the non-toxic cystathionine, and thereafter into cysteine and alpha-ketobutyrate. These conversions require pyridoxal-5'-phosphate, the active form of vitamin B6. B
Methyl groups are necessary for the synthesis of: DNA, RNA, choline, betaine, adrenaline, noradrenaline, serotonin, carnitine and creatine. Cardiovascular Disease Homocysteine itself is a highly toxic substance, especially to the vascular walls. McCully was the first who recognised the significance of this.13 Clarke et al. mentions hyperhomocysteinemia as an independent risk factor for vascular disease.14 Conversion of homocysteine to less toxic forms such as methionine and cystathionine protects the vascular walls against the pathologic effects of homocysteine. The active forms of folate and vitamin B assist in the conversion of homocysteine into methionine; the active form of vitamin B6, pyridoxal-5'-phosphate, converts homo-cysteine into cystathionine (transsul-furation pathway). Therefore, the conversion of homocysteine is mainly dependent folate, vitamin B12 and vitamin B6. Ubbink et al. showed clinically that there is a relationship between hyperhomocysteinemia and lower plasma concentrations of pyridoxal-5'-phosphate, cobalamin and folic acid. Homocysteine levels could be lowered by a supplement with 10 mg pyridoxal, 1 mg folic acid and 400 mcg cyanocobalamin. They stated that appropriate vitamin therapy may be both efficient and cost-effective to control elevated plasma homo-cysteine concentrations.15 This conclusion was drawn for the prevention of occlusive vascular disease. Neuropsychiatric Disorders In 1988, Lindenbaum et al. published in the New England Journal of Medicine findings of 141 elderly patients with neuropsychiatric disorders.16 In 28% of these neuropsychiatric patients, there was no anemia or macrocytosis. Only 16% had abnormal low serum B12 levels. Every patient in this group benefited from cobalamin therapy. In those who had elevated homocysteine levels, the homocysteine level decreased. The findings of Linden-baum were confirmed by Naurath et al.17 who performed a clinical trial on a group of 285 elderly persons with an injection containing 1 mg vitamin B12, 1.1 mg folate and 5 mg vitamin B6 versus placebo. Among other metabolite assays, homo-cysteine levels were measured. The conclusion of the authors was: “The response rate to vitamin supplements supports the notion that metabolic evidence of vitamin deficiency is common in the elderly, even in the presence of normal serum vitamin levels. Metabolite assays permit identification of elderly subjects who may benefit from vitamin supplements.” Normal serum vitamin levels included that of vitamin B. 12 NTD: More than Folate In 1995 Mills et al. demonstrated hyperhomocysteinemia in pregnant women.18 They suggest that the most effective periconceptional prophylaxis to prevent neural tube defect may require vitamin B as well as folic acid. With the underlying pathophysiology in mind, improvement of the methylation process, which includes lowering of the homo-cysteine level, may be the clue to lowering the risk of babies with NTD. Goddijn et al. find that hyperhomocysteinemia is a risk factor for placental abruption.19 In women Folate and Neural Tube Defect Risk with this disorder, they also find low levels of folic acid, vitamin B12 and vitamin B6. Other Disorders Serum homocysteine level is a significant predictor and indicator for many disorders: cardiovascular disease; neurological disorders, including paresthesia, sensory loss and ataxia; psychiatric disorders, including depression, dementia and schizophrenia; anemia; and the birth of babies with NTD. It may be postulated, on the basis of current research, that hyperhomocysteinemia and a disturbed methylation may also be involved in other disorders such as the birth of babies with orofacial cleft, carpal tunnel syndrome, asthma, multiple sclerosis, cervix carcinoma, other types of cancer, and thrombosis risk groups may be the elderly, vegetarians and stomach patients (vitamin B12 deficiency) expectant mothers, anticonvulsant users (require extra folate), and oral contraceptive users. A very recent epidemiologic study in Norway shows that coffee, filtered or boiled, elevates homocysteine levels.20 There is a dose-response relationship. Smoking in connection to drinking coffee shows even higher elevations. Tea does not produce this effect. No Alternative Allopathic Treatments It is clear that lowering of homocysteine levels is a crucial element in preventing and curing disorders. Treatment is a combination of folic acid, vitamin B12 and/or vitamin B6. The variety of disorders and the combination therapy of three B-vitamins constitute a proper model for orthomolecular medicine. So far, no alternative allopathic medication is available to this orthomolecular treatment. This precedent provides a good opportunity for the orthomolecular medical discipline to prove its efficacy in the daily practice of many physicians and is a firm step forward in achieving the new paradigm. As Abram Hoffer is often quoted, it takes forty years to get a new paradigm accepted. This prerequisite is now fulfilled. Journal of Orthomolecular Medicine Vol. 13, No. 1, 1998 References
pregnancies complicated by neural tube defects. The Lancet, 1995; 345:149-151. 19.Goddijn-Wessel TAW et al: Hyperhomo-cysteinemia: a risk factor for placental abruption or infarction. Eur J Obst Gynecol Repr Biol, 1996; 66: 23-29. 20. Nygard O et al: Coffee consumption and plasma total homocysteine: the Hordalund homocysteine study. Am J Clin Nutr, 1997; 65: 136-143. |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)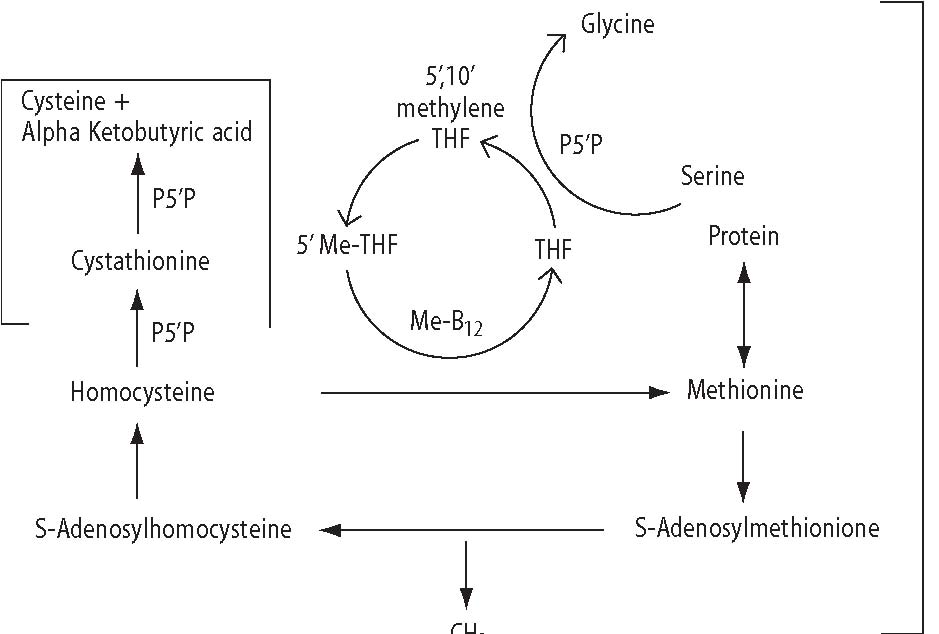 A
A