 |

|
|
|
|
 Back to 1998 1st Quarter Table of Contents
Back to 1998 1st Quarter Table of Contents
All new patients seen at The Center must complete a nutrition evaluation questionnaire as part of their application packet. This questionnaire is the Sherlock Questionnaire containing 318 different food and drink items. For seven days, the patient, or parent in case of children, places a mark beside each serving of food or drink consumed. Blank spaces are available to write in any items not listed on the questionnaire. The information is entered into a computer program which calculates the percentage of the RDA from selected nutrients and prints out a nutrition evaluation summary. One obvious problem in using the information from the questionnaire is that one must be conscientious in keeping accurate records of all food and drink consumed. It has been our experience that patients coming to The Center are very conscientious and interested in their health and do a very good job with the questionnaire. One control available as a check on the nutrition information is the results from the various vitamin and mineral laboratory tests performed on the patient’s urine, hair, erythrocytes, leucocytes and plasma. One case will be presented demonstrating the value of the nutrition questionnaire. The patient is a 10 year-old white male with major complaints of attention deficit disorder (ADD) and obesity. Other complaints included insomnia, anger, and headache. His height was 58.5 inches and weight was 130 pounds (His calculated ideal weight is 95 pounds). He was diagnosed with ADD in 1994 and takes Ritalin™ daily. The summary of his nutrition evaluation questionnaire is shown in Figure 1, p.29. Fats represented 32.6% of calories, carbohydrates were 54.6% with 18.7% of these being from refined carbohydrates. Some of the items recorded on the seven day profile included the following servings: 1 TangTM, 4 soft-drinks, 6 unsweetened grape juice, 1 orange juice, 1 grapefruit juice, 1 pineapple juice, 15 different vegetables, 3 of potato chips, 1 fish sandwich with Tartar sauce, 2 of Rice KrispiesTM, 10 of saltine crackers, 1 of TriscuitTM crackers, 5 of popcorn, 1 of chicken, 2 of chili with meat, 1 of baked beans, 3 hamburgers with bun, 3 of french fries, 3 slices of pizza, I of Cheerios.TM This list of foods could help explain the problem with obesity. A cytotoxic sensitivity test for adverse food sensitivities1 was ordered as part of the laboratory work-up. The results were interesting considering the foods consumed by this patient. He showed the following cytotoxic reactions. Plus 1 (1+): American cheddar and mozzarella cheese, avocado, broccoli chocolate, corn, dextrose, fluorine, grapefruit, oat, orange, rice, tomato, vanilla, Brewer’s yeast, MSG, yellow dye and lemon, In all, the patient was sensitive to 35 different substances out of a total of 90 tested. Note that the sensitivities almost mirrored the types of food consumed. With these many food sensitivities, it is not unexpected that child’s attention would wander. It is our experience that many children with ADD or ADHD (attention deficit hyperactive disorder) have adverse food reactions. He also had a “O” urine vitamin C level and 28 The Nutrition Evaluation Questionnairre as a Diagnostic Aid Figure 1. Nutrition Evaluation Summary Nutrition Evaluation SUMMARY #3369 09/02/97Age: 10, Sex: M HT: 58 in, WT: 130 lb Nutrient Average % RDA* RDA Daily Intake 0 100 200 300 Ascorbate 192.0 mg Thiamine 1.8 mg Riboflavin 2.1 mg Niacin 21.6 mg Pantothenate 3.6 mg Pyridoxine 2.2 mg Folacin 303.0 mcg Vitamin B12 8.0 mcg Biotin 31.0 mcg Vitamin A 20631.0 IU Vitamin E 7.1 IU Vitamin K 79.6 mcg Calcium 965.0 mg Iron 20.7 mg Magnesium 294.0 mg Phosphorus 1303.0 mg Potassium 3043.0 mg Sodium 3664.0 mg Zinc 5.5 mg Copper 1.1 mg Manganese 2.3 mg Selenium 50.3 mcg Iodine 68.0 mcg Energy 2107 kcal Fats 77.8 g Llnoleic Acid 9.4 g Carbohydrates 296.1 g Natural Carbs 194.7 g Refined Carbs 101.4 g Sugar 40.7 g Fiber 7.5 g Protein 69.7 g Coffee + Tea 0.0 cups Alcohol 0.0 drinks Cal/Phos 0.7 ratio Potass/Sodium 0.8 ratio 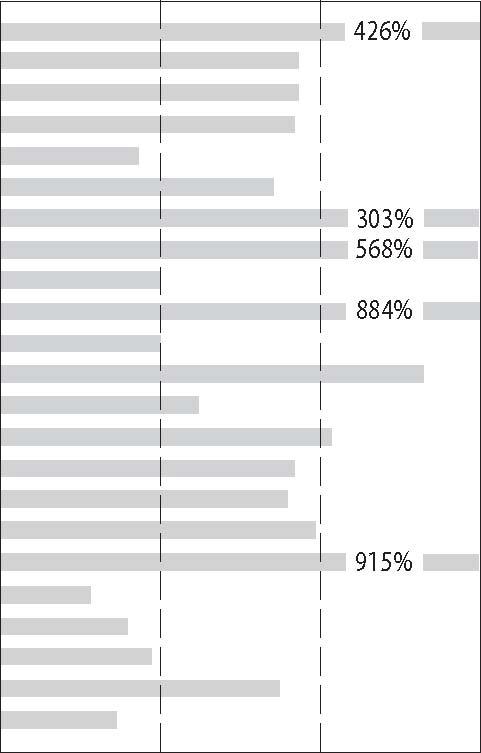 45.0 mg 1.0 mg 1.2 mg 13.0 mg 5.0 mg 1.4 mg 100.0 mcg 1.4 mcg 30.0 mcg 2330.0 IU 7.0 mcg 30.0 mcg 800.0 mg 10.0 mg 170.0 mg 800.0 mg 1600.0 mg 400.0 mg 10.0 mg
30.0 mcg 120.0 mcg (32.6% of calories) (54.6% of calories) (35.9% of calories) (34.2% of calories & (18.7% of calories)) (12.8% of calories) (0.0% of calories) *The RDA’s are estimates based on values and ranges published by the FDA and the National Research Council. 29 Journal of Orthomolecular Medicine Vol. 13, No. 1, 1998 an elevated urine pyrrole.2 Plus 2 (2+): Apple, banana, carrot, cottage cheese, fructose, honey milk, cow peach, saccharin, tobacco, Baker’s yeast, coffee Plus 3 (3+): pineapple Other laboratory tests, including thyroid function, were normal. It is important to check patients with ADD or ADHD for thyroid dysfunction. A study published in a 1993 issue of Pediatrics found abnormal thyroid function tests in 14 out of 277 children with ADHD. It concluded that the prevalence of thyroid abnormalities were 5.4% higher in ADHD patients. As mentioned above, this patient had an elevated urine pyrrole. High pyrrole excretors tend to lose zinc and vitamin B6 in their urine. These patients also usually have a low hair tissue zinc and are high in hydroxyproline.2 Also of interest, (and a good check on information on the nutrition profile) his measured urine potassium to sodium ratio (0.9) matched the ratio calculated from the nutrition profile (0.8). The acute medical model dictates that a child with ADD or ADHD must require medication to suppress unwanted symptoms. At The Center the question is asked, “Why is this child climbing the walls, being obnoxious, unable to focus attention, and having all the behaviors parents face with this burden and endure to the point of total exasperation?” One of the authors (HDR) has four decades of evaluating and treating hyperactive children, and we understand something of the biochemistry of behavior. We do know that ADD is not a RitalinTM or medication deficiency! We have found that adverse food reactions, hidden yeast problems, trace mineral imbalances, specific nutrient deficiencies, parasites and various metabolic disorders, as well as emotional factors are involved in attention deficit problems.3 One should not rush to label children with an alphabetic label. As stated in the Kellogg Report in 1980, “When children who exhibit learning and/or behavioral disorders are examined by a number of specialists, the diagnosis is more closely related to the orientation of the specialist than it is to the essential problem facing the child.” Children who have been seen by eight different specialists, commonly have eight different diagnoses, ranging from hyperactivity to dyslexia to autism. These diagnoses do not indicate the cause of the problem, and do not suggest any specific treatment. As Abram Hoffer, M.D., Ph.D., a pioneer in orthomolecular medicine wrote in 1966, “If we do not try to improve the nutrition of our children, not only children suffering from ADD, but also of almost every child in our high-tech society, we can look forward to another millennium of chronic illness, perhaps so severe as to threaten the species.” How did the patient in this case respond to treatment? In light of his “O” urine vitamin C, he was given a high-dose vitamin C treatment. Vitamin C is very effective in treating allergy symptoms as it tends to stabilize the membranes of tissue mast cells and basophils. The parents were advised about diet modification and restricting or eliminating the reactive foods identified in the cytotoxic sensitivity test. A follow up visit about two months later showed a slight weight loss of three pounds. The parents reported a big change in his behavior: his anger was gone, he was sleeping more, his concentration was better and he had improved in his school work. He continues to be followed at The Center. References
|

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)