 |

|
|
|
|
 Back to 1997 1st Quarter Table of Contents
Back to 1997 1st Quarter Table of Contents
Since the l970s, and perhaps even earlier, America has been suffering the effects of an epidemic pathological phenomenon eating away at the very core of our society. Virtually everyone is alarmed; we make new laws, build more jails and spend billions of dollars a year, and yet the sex offender (paraphilia) epidemic continues to expand exponentially. In this article, we will explore why this epidemic has ocurred, and what to do about it. We will discard old-fashioned, ‘good intention’ type therapeutic approaches and arm chair speculations for a modern biomedical model for these devastating disorders. We will abandon the criminal model and move toward a biomedical model. A neurobiological model of obsessive-compulsive paraphilia (OCP) is essential in the effective diagnosis and treatment of these disorders. The pathophysiological model is essential in medical practice as it provides an understanding of clinical symptomatology and a rational basis for therapeutic intervention, a model that is missing in the diagnosis and treatment of paraphilialogicaldisorders,whichrelieson a hodgepodge of good intentions rather than on a rational biomedical model. In fact, there is no established model or rationale for the diagnosis and treatment of these highly resistant and debilitating disorders. It is the author’s primary intention to develop a biomedical diagnostic and treatment model in this article, to begin a rational seminal effort, which will hopefully be continued by others. An explanation for the clinical manifestations and the therapeutic response of different interventions of an illness based on the anatomy and physiology of the disease is essential in the clinical practice of medicine, and should extend to the psychiatric and psychological specialties as well. Paraphilialogical disorders have been considered to be a type of CNS pathology similar to other biological pathological states. The central nervous system (CNS) is believed affected by the disorders that we shall call OCP, however, the DSM IV does not contain the OCPnosologyatthistime. The author is using this term as a hypothetical term to explain symptoms which, from many years of personal clinical experience, appear similar to OCD. DSM IV lists several forms of paraphilic disorders such as masochism, sadism, voyeurism, exhibitionism, and pedophilia. 1 Some types of sexual fetishism may also be classified as paraphilia. Only two of them will be described in this article. In this article we will address only rape (or raptophilia–the sexual arousal and orgasm maximized by force and humiliation), and pedophilia (sexual attraction to children). Each paraphilia is unique because it is fused or encoded to a particular sexual erotic ritualistic behavior, or object, as a contingency requirement for maximum sexual gratification, which is socially and legally unacceptable.2 Another feature of paraphilic disorders is that the fantasy or ritual attack may occur several times in a very ritualistic fashion during sexual arousal, or as part of the foreplay leading to sexual erotic arousal and ultimately orgasm.3 In more than a decade of clinical research, the author has catalogued some thirty different paraphilias, each with content specific rituals and behaviors in the service of sexual erotic arousal and orgasm. The repetitive,ritualistic behaviors of para-philiaare very similar to the uncontrollable rituals observed in obsessive-compulsive disorder (OCD). An important difference between OCP and OCD is the component ofsexual stimulation and orgasm seen with OCP that is not found in OCD.4 Like patients suffering OCD, OCP patients often hav eco-morbidpersonality disorders and or other medical condition swhich also require appropriate professional attention, perhaps simultaneously.5 Thus, it appears fairly reasonable to assume there may be anatomical similarities between OCP and OCD, such that models proposed for OCD may help explain OCP. On clinical grounds,theauthorhypothesizesthatOCP is one of the spectrum of OCD disorders.6 Because there are putative neurobiological models of OCD, an attempt will be made to apply current knowledge about OCD to OCP.7,8 Our discussion will be divided into several parts. First, a comparison will be made among the clinical manifestations of OCD and OCP. Next, an integrated hypothetical neurobiological model of OCD will be presented. It will then be shown how the phenomena of OCP may be sharing similar neurobiological systems as OCD. Finally, the difference between OCP and OCD will be discussed with particular reference to serotonin, obses-sion, compulsion, faulty cognition and orgasm. Clinical Comparisons Between OCP and OCDAccordingtoDSMIV,acompulsionis defined as a ‘ritualistic behavior’, or mental act that the person feels driven to perform or think,regardless of normallogicorreason.9 In this author’s clinical experience, when individuals suffering paraphilic disorders are questioned as to how they would de-fine their behavior, the above definition fits quite well. As with compulsions and obsessions, the behavior of the paraphiliac contains content-specific rituals with well-defined mental or behavioral sequences. Because of the apparent similarities between the paraphilias and OCD, it may be possible to understand why an other-wise ‘reasonable’ individual who operates fairly rationally in other aspects of his life will act irrationally to a particular sexual-erotic stimulus.10 Elsewhere, it has been stated that the content-specific rituals of OCD seem like pre-packaged sequences of behaviors that are executed upon trigger by a stimulus. These ‘prepackaged’ sequences seem similar to computer programs known as macros.11 For example, the compulsive hand washer is driven to access the macro of his hand-washing ritual by a trigger such as a handshake, due to some experi-entially encoded fear of ‘contamination’. The encoded fear of ‘contamination’ cre-ates anxiety which is adysphoric emotional state temporarily relieved by the obses-sive-compulsive ritual.. Anxiety may be defined as a psychophysiological state of dysphoria produced by an encoded fear to a particular bio-socialstimulus.12 The design of the macro is based on past experiences relating to, or associated with,‘contamina-tion’ from handshaking, touching sticky surfaces, or other ordinary daily rituals involving touching objects. Thus, encoded fears and the counter rituals that are developed to deal with them seem irrational to all but the patient. This suggests a dual nature to obsessive-com-pulsive behavior, the obsessive fear and the compulsive act. The fear seems to create the anxiety, while the act is an effort to counter it. As will be explained later, most obsessive-compulsive fears are fused or coded molecularly to the rituals, such that any bio-social stimuli in the repertoire of possible bio-social codes will trigger hand washing rituals in the manner of a macro which seems autonomic. This seems true because patients avoid triggers of obses-sional fears knowing that rituals will come in their wake.13 Paraphilias present with similar irrational rituals as OCD. At the core of any paraphilia is usually some type of encoded doubt or fear combined with some form of ritualistic sexual behavioral though para-philic rituals can, and often are, encoded solely for sexual arousal and orgasm. For example, in one patient in the author’s ex-perience, a compulsive exhibitionist had a fear that he was inadequate in adult hetero-sexual intercourse, so he said, but derived great sexual gratification from shocking and causing fright in unsuspecting females whom he found sexually attractive. Orgasm reduced all anxiety over any subjective sexual inadequacy.14 In paraphilic exhi-bitionism, sexual arousal was apparently fused to the act of genital exhibitionism in front of unsuspecting female targets. The shock and surprise component generates intense sexual orgasm for the exhibition-ist as he views the shocked response of the victim. The ritualized sequences of behavior that have been previously termed a Macro for OCD seem to exist for the paraphilialogical disorders, the difference being sexual themes. In a compulsive rapist, there appears to be an obsessive craving toward the target that requires stalking and attack-ing rituals. The sexual-erotic contingency requirement for the raptophile (rapist) is violence, torture, pain, and humiliation of the target victim. Some raptophilic ritu-als include murder or injuring the target victim physically or emotionally, in order to achieve orgasm. For the purpose of this paper, the macro or ritualized sexual behavior re-sponds to a well-defined sexual-erotic design defined as a “Sexual-Erotic Arousal Pattern,“ or SEAP. This is similar to the ritualized compulsive behavior, or macro, of OCD, minus the sexual-erotic compo-nent. For the rapist, the compulsive SEAP is accessed as an orgasmic ritual in response to sexuo-erotic craving. For a pedophile, a arousal and orgasm is achieved at the sight of certain kinds of children. Under such circumstances, the pedophilic SEAP isaccessedwhenthetargetentersthevisual field and the pedophile goes into an obses-sive-compulsivecravingmode,stalkinghis target, masturbating often several times a day. The author has quantified pedophilic craving in several chronic pedophiles on the modified Y-BOCS (Yale Brown Ob-sessive-Compulsive Scale, range 0 to 40). They invariably fall in the high thirty range, an extreme measurement. However, the pedophilic craving may be very successfully reducedwithcertainSSRI(selectiveseroton-ergic reuptake inhibitors) –as demonstrated in some pilot trials. The Macro and the SEAPIt has been shown clinically, that pa-tients with OCD have a high incidence of parents who suffered from panic disorder and other types of anxiety disorders often never diagnosed or treated.15 During development, such children are probably hyper-sensitized to the environment in a fear-based manner due to excessive parental encoding of fears, doubts, and paranoid types of cognitions. Such children adapt bio-socially by creating rituals based on various behaviorally encoded exposures that are associated with,or fused to,fears,doubt and suspicion.It is likely that theparaphilic disorders are potentiated by bio-social sexual-erotic exposures in juvenile life. It is also possible that genetic proclivities may come into play in yet unknown ways. The following example, from the de-tailed sexual history of a compulsive rapist will illustrate this. This rapist had, in early life, witnessed first hand violent sexual behavior between his mother and several of her consort lovers which became fused (encoded) as preferred sexual-erotic arousal. Such visual exposures are believed to become coded neurobiologically as the Sexual-Erotic Arousal Pattern (SEAP). Thus, toxic child-hood sexual exposures appear to become fused (via molecular encoding) with the violence and brutality creating a SEAPinan analogous fashion similar to the phenomena of imprinting.16, 17, 18 The basis for the concept of the SEAP as a molecularly encoded behavior can be shown from recent neurobiological research. In Aplasia ( a species of shrimp) long term synaptic modulation requires synthesis of new macromolecules. (serot-onin molecules are suspect).19 This has also been confirmed in higher orders of species wherelearninginvolvesthe denovo forma-tion of molecules and neural pathways.20 In addition, it has been demonstrated that neuroreceptorchangesoccurinresponseto social exposures.21 In this regard, a neural mechanism for plasticity in the human cortex has been postulated. The neural architecture of the cortex is susceptible to experience-dependent modifications dur-ing development that can result in lasting changes in adult neural architecture.22 MRI studies have demonstrated a positive relationship between severe emotional trauma and changes in the structure of the hippocampus,23 akey neuro anatomical region in our discussion. Thus, the author postulates that sexual-erotic trauma, force, adventitious exposure, or simple visual exposure in childhoodmaycreatebiochemicalchanges in the brain. This hypothesis is the neuro-biological basis for the SEAP. Such SEAP like Macros may exist for both OCD and OCP disorders, molecularly encoded programs or templates of behavior that have been neurally imprinted into the cel-lular memory of the brain.24 Supportive clinical evidence that such programs may in fact exist and be encoded and stored in the temporal lobe, as well as other brain areas, comes form several sources. Patients with the Kluver-Bucy syndrome, a temporal lobe abnormality, exhibit hypersexuality and hyper-orality. Also, when the temporal lobe is stimulated in the fully conscious epileptic patients, complex visual and auditory images are stimulated, some with strong sexual and emotional themes. In addition, during an attackoftemporallobeepilepsy,thereisinten-sification of these kinds of reactions 25. From thisevidence,itseemsentirelypossiblethat all, or part, of SEAPS and OCD programs may be housed or modulated by temporal lobe neurobiological systems. Putative Neuroanatomy The temporal lobe is in a crucial neuroanatomic site when viewed in the context of a bio-medical model of anxiety and obsessive-compulsive disorders. One model of anxiety postulates a system that inhibits ongoing behavior in the presence of certain stimuli, such as danger, pun-ishment, non-reward, novelty or innate fear. In anxiety disorders (and perhaps in paraphilicdisorders),thesesystemsmaybe hyper-sensitive or defective in some way; in particular the serotonergic transmitter subtype 5-HT1 (5 hydroxytryptamine). Thereareaboutsomesevenknownfamilies of serotonergic transmitters and fourteen subtypes, the one (A) sub type seems to play a principle role in OCD and the other anxietydisorders.Theauthorhypothesizes that OCP may be part of the spectrum of disorders of OCD’s, since experimen-tal pilot trials with certain SSRIs yields positivereduction,especiallyinpedophilic craving. The behavioral inhibition system (BIS) is thought to access behaviors that will cope with stimuli26 described above. The BIS is a septal-hippocampal system that accesses behavioral programs from the temporal lobe; the putative anatomi-cal location of SEAP programs. Also, in a recent theoretical model of OCD, it is thought that there is a circuit within the prefrontal cortex-basal ganglia-thalamic which perseverates motor behavior.27 Here the BIS may offer the link between access of the SEAP from the temporal lobe and its motor execution through connections to the prefrontal cortex-basal ganglia-thalamic circuit via the Papez circuit.28 The reader is reminded again that these are hypothetical speculations which are designed to stimulate further exploration, not intended to confirm causation. In this next section, we will attempt to link all three neuroanatomic systems by followingamotorprogram,orSEAP,from its hypothetical storage in the temporal lobe to its perseverated motor execution. It should be kept in mind that both the SEAP and the macro are variations of a normal neuropsychological process. Ac-cordingtoourmodel,theBISfunctionsin allindividualstoprovidepre-programmed encoded behaviors designed to cope with anxiety-producing stimuli, a fight or flight pattern, and, in our model; comorbidly coded sexual arousal behaviors (paraphili-alogical disorders). If pathologically coded, the macro or SEAPbehaviorperseveratesuncontrollably. This repetition may result from neuro-chemical dysfunction; a good candidate is the 5-HT1 subtype and/or neuro anatomi-cal impairment in the BIS, the prefrontal cortex-basal ganglia-thalmic circuits or other combinations. Other transmitters could also be affected pathologically by cascadingeffects,becausethehumanbrain is currently known to have some two hundred transmitters and neuromodula-tors, all of which have been cloned. It is not likely that any single transmitter or modulatorfunctionsalone,eithernormally or pathologically. The BIS is a system that modulates anxiety from stimuli that ‘warn of punishment’ or ‘non-reward’ novel stimuli (sexual arousal) and innate fear stimuli. The BIS will react through inhibi-tionofongoingbehavior,increasedlevelof arousal and attention to the environment, especially to novel stimuli. The anatomi-cal structure of the BIS is shown in Figure 1(Page 34).29 ThefollowingisasummaryoftheBIS taken from Grey.30 It includes the septal area, the hippocampal formation, Papez circuit(Figure2,Page35)whichrunsfrom the subicular area in the hippocampus to the mammilary bodies, anterior thalamus, cingulate cortex, and back to the subicular area and neocortical inputs to the septal-hippocampal system from the entorhinal area and prefrontal cortex. These structures are supportive of the author’s hypothesis. There are dense populations of ascending noradrenergic and serotonergic inputs to the septo-hippocampal system; dopamin-ergic input to the septo-hippocampal system; noradrenergic innervation of the hypothalamus and, possibly descending noradrenergic fibers of the locus coeruleus that may also be involved in transmitter cascading effects. Itappearsthatthesepto-hippocampal system along with the entorhinal area and the‘subicularloop’(Papezcircuit)havethe task of predicting sensory events to which theorganismwillbeexposedto.Sexualand eroticstimulationcanbeclearlyinterpreted as a sensory event. If there is a coded mismatch between actual and predicted events, or if the predicted event is aversive, strategies involving alternative responses will be tested, which are attempts to assist the organism to cope. The BIS is believed to produce attention to and exploration of the environment which is executed via the entorhinal area and the cingulate cortex and behavioral inhibition via the cingulate cortex and a descending projection from thelateralseptalareatothehypothalamus. The hippocampal theta rhythm is believed to quantify and pace the flow of informa-tion around this system. It is particularly interesting for our theme that the theta rhythm is strongly influenced by the effect of testosterone on the locus coeruleus which results in a decreasedthresholdforproductionoftheta rhythm with resulting increase in flow of information around the BIS.31 The prin-ciple role of the noradrenergic projection to the septo-hippocampal system is to tag stimuli as ‘important’ and requiring particularattention.Aswehavementioned earlier, the ascending projections in this area are particularly innervated with se-rotonergic projections and if cross coded by pedophilic or other paraphilic macros, sexual and erotic functions may become obsessive and compulsive. The prefrontal cortex has two princi-ple roles. First, it transmits to the septal-hippocampal system information about 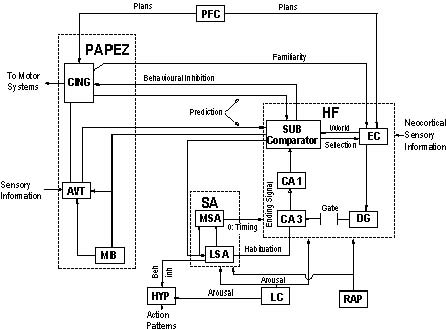 Figure 1. Summary of the Behavioural Inhibition System according to Grey. The three major building blocks are shown in bold print: HF, the hippocampal forma-tion, made up of the entorhinal cortex, EC, the dentate gyrus, DG, CA3, CA1, and the subicular areas, SUB: SA, the septal area, containing the medial and lateral septal areas, MSA and LSA; and the Papez circuit, which receives projections from and returns them to the subicular area via the mamilliary bodies, MB, anteroventral thalamus, AVT, and the cinguate cortex CING. Other structures shown are the hypothalamus, HYP, the locus coerulus, LC, the raphe nuclei, RAP, and the prefrontal cortex, PFC. Arrows show the direction of projection; the projection from SUB to LSA lacks anatomical confirmation. The term “beh inh” is behavioural inhibition. ongoing motor programs to be used in The symptoms of obsessive anxiety are the processing of predicted sensory events. believed to arise from excessive activity in Secondly, it facilitates control by the the BIS which appears related to 5-HT1 neocortex of verbally coded information activity. In particular, obsessive-compulsive (that is believed to be stored in macro mol-symptoms seem due to hyperactivity by the ecules). The most likely area for the stor-BIS which probably results from interac-age of sexual-erotic and anxiolytic Macro’s tions of the septo-hippocampal system [molecularly encoded] is the temporal lobe and the neocortex. Anxiolytic compounds, which is accessed by the septo-hippocampal especially the SSRIs are effective in anxiety system through pathways to the entorhinal disorders because they modulate and nor-area, and perhaps to other adjacent areas. malize the activity of ascending noradren-There appears to be a functional interaction ergic and serotonergic projections to the between an encoded SEAP and an OCD septo-hippocampal system. Macro, probably in the temporal lobe and It is hypothesized that these projec-the neocortex once an encoded program tions contain molecularly coded informa-has been accessed. tion (possible 5-HT2 and other sub types of 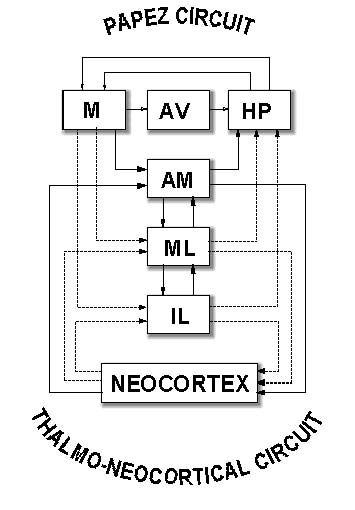 Figure 2. Interaction between the Papez circuit and thalamo-neocortical circuit This model is a representation of the interaction between the Papez circuit and the tha-lamo-neocortical circuit where AM is the antero-medial nucleus of the thalamus; HP is the hippocampus; IL is the intralaminar nuclei of the thalamus; M is mamilliary body; and ML is the midline nuclei of thalamus. 5-HT transmitters). It is also believed that thereisaninteractionbetweentheneocor-texandthesepto-hippocampalsystemthat suggests participation of the neocortex in anxiety disorders, obsessive compulsive symptoms including our hypothetically new category of obsessive-compulsive paraphilialogical disorders. This proposed neocortical dynamic will be described in the next section of this paper. The contribution of the neocortex and the frontal lobe are particularly in-fluential in the process of cognition. It is believedthatsocialinhibitionandconcern over the consequences of actions as well as impulse control are functions of this area.32 During obsessive-compulsive ritual behavior there seems to be a loss of frontal lobecontrolwhichhasbeensuggestedtobe related to defective or hypermetabolism of themedialorbitalgyrusofthefrontallobe. These dynamics are fairly well established and they are believed to involve 5-HT1 and possibly other 5-HT families of syn-aptic dynamics. This area seems to rivet a pathologicalmacro(orparaphilicSEAP)at the expense of impulse control. This area is termed the ‘worry circuit’ of the frontal lobe.33 Once a macro or SEAP is encoded or riveted into the ‘worry circuit’ (Figure3 page 37), it undergoes perseveration of both thoughts and behavior. It appears that a hyper-metabolic BIS continuously repeats the encoded program of the macro or SEAP . In clinical practice, it is because of these neurodynamics that the patient continually repeats checking behaviors for fear of ‘doing something not right’. This is why obsessive compulsive disorders are often referred to as ‘doubting disorders’. Theparaphilicpatientknowsperfectlywell that his paraphilic craving is increasing, but “can’t” stop it. Once obsessive craving occurs the patient is completely oblivious tolaws,consequencesorjailsentences.For this reason, some authors have applied the term ‘paraphilic attack’ to the full blown paraphilic episode. Because it is similar to an epileptic attack, when it occurs the patient is completely powerless to stop it. Theroleofthemalesexhormone,tes-tosterone, may now be discussed in OCP. As mentioned previously, testosterone primesthelocuscoeruleustoincreasetheta waveactivityintheBISwiththeresultthat it increases circulation of messages around the BIS. It is believed that during sexual arousal, there is rapid processing of infor-mation around the BIS, which is believed to trigger SEAP access. The terminal point for paraphiles is sexual orgasm, because of the powerful endorphin reward which reinforces the behavior.34 It should be noted here that the BIS is thought to be hyperactive especially in regard to 5-HT1 transmission in obsessive-compulsive and other OCD spectrum disorders35 which may add to the likelihood of the repeti-tion of information circulating through the BIS. The system appears to function as though thoughts and behavior proceeds toorapidly,resultinginbehavioralstaccato typestartingandstopping,orcheckingand re-checking. The question now arises as to why testosterone (a sex hormone) would increasearousaloftheBIS.Asstatedearlier, innatefearstimuli’especiallythosethatare encoded during juvenile socialization, will stimulate BIS arousal.36 For example, in a rapist, pictures or live female “targets” with certain kinds of angry faces may increase anxiety and sexual erotic craving simulta-neouslybecausetheyareneurobiologically coded that way. By contrast, in pedophiles the same sequence is believed to occur, the only difference is the coding of a child target. It is also interesting to note that lesions of the locus coeruleus will increase gregariousness (in rats) which is likely due to reduction in avoidance produced by the stimulus.37 Thus, it is postulated that during sexual arousal, testosterone will increase in the BIS and may access any other co-morbidly coded program,(i.e. an obsessive-compulsive paraphilialogical arousal pattern such as the SEAP). Ithasbeenproposedthatsexual-erotic stimuli coded in the course of dominance and socialization interactions are among the kinds of stimuli which activate the BIS.38 Assuming that sexual behavior is such an interaction, then stimuli coded in the course of such social exposures are among the kinds of stimuli that will acti-vate the BIS, provided such stimuli have beenencodedmolecularly(bysexualerotic exposure) or ‘fused’ to the interaction. Duringsexualarousal,(sexual-eroticmatu-ration) the dominance of social interac-tions are believed to be fused to paraphilic sexual rituals. Thus, paraphilic encoding is assumed to cause the programmed, encoded BIS to access whatever SEAP, or in some cases multiple SEAPS, that it has been coded for. During sexual-erotic arousal, a ‘nor-mal’ heterosexual male manifests a crav-ing for peno-vaginal penetration which is bondedtoaffectionor‘love’andproducesa reciprocalcravinginthefemalethatresults in mutual sexual-erotic and emotional satisfaction. However, if a response such as anangryfaceandaggression,orviolence,is encoded, then the sexual-erotic ritual and behavior may induce rape behavior. Such encoded programs are consistently seen in Figure 3. Proposed model of Brain System Dysregulation that mediates the symptomatic expression of OCD 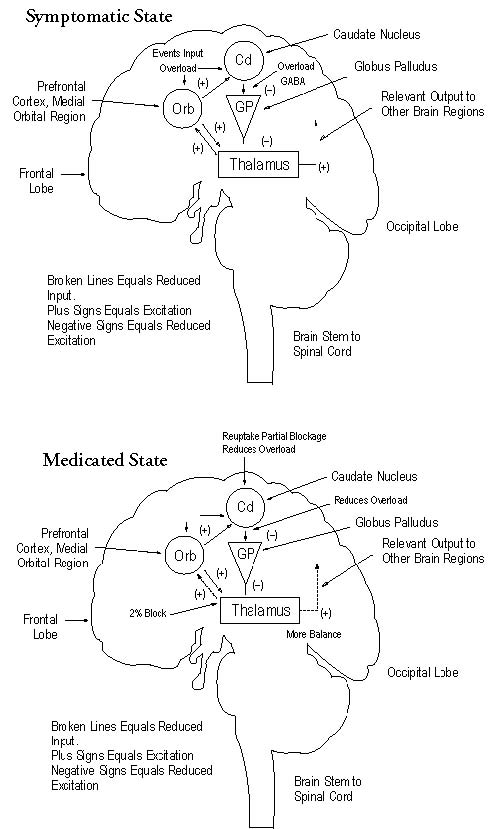 Adapted fromBaxter, JR, Jr.; Schwartz, J.M.; Bergman, KS; Caudate glucose metabolic rate changes with both drug and behaviour therapy for Obsessive Compulsive Disorder. Archives of General Psy-chiatry 1992; 49: 681-689. raptophiles, especially multiple exposures to brutal, violent sexual acts witnessed by mothers and paramours, or other kinds of experiences of a similar nature by other relatives, adults or possibly adolescent fe-males. The final adult rape ritual pattern then comes to rest in the adult SEAP of the typical raptophile when a craving for a greater sexual-erotic response begins. Once the paraphiliac SEAP is trig-gered in an individual with an encoded compulsive paraphilia, it is believed that the SEAP will perseverate in the ‘worry circuit’ of the frontal lobe until orgasm terminates the sexual-erotic ritual. Un-fortunately, the SEAP ritual or rituals becomes the end point, because it receives positive reinforcement through orgasm. During the beginning stages of sexual arousal, the paraphiliac patient begins to scan for these associated encoded stimuli in the environment until a match is made, which ultimately accesses the full-blown SEAP program. Because the frontal lobe may be in a state of 5-HT2 hypermetabolism and is fully occupied during a paraphiliac at-tack, uncontrollable release of the SEAP occurs.39 There is, thus, a complete loss of impulse control until orgasm completes the ritual. Once orgasm is reached, the patient can regain impulse control, inhi-bition is restored and a profound sense of dysphoria overwhelms the patient, known commonly as guilt. In the author’s experi-enceofmanyyears,paraphilesneverreport guiltfeelingsduringtheirparaphilicrituals, only afterward, and usually only after they are caught. The guilt comes from being caught, not from the paraphilic ritual behaviors. One possible core reason why theobsessivecravingissouncontrollableis thatitmaybedrivenby5-HT2dysfunction whichseemstobecommontootherOCD and spectrum disorders.40 Clinical CorrelationA comparison may now be made to the original concept that obsessive-compulsive behavior is designed to reduce anxiety co-morbidly encoded with para-philic disorders. In some paraphilias like raptophilia(rape),sadism,anger,violence, torture, and various types of brutality are codedinthesexual-eroticequationandare required for greater arousal and orgasm. Because of its coding and relationship to probable5-HT2dysfunction,thisbehavior can become obsessive and compulsive. In addition,becausefearandorcombinations of the above the obsessions are reinforced by sexual orgasm, the craving to act on the paraphilic obsession becomes virtually ir-resistible. Thus paraphilic SEAP rituals are a means to change any form of dysphoria or anxiety to euphoric orgasm. This cre-ates a pathological condition in which the craving for sexual targets is obsessively and compulsively stalked in order to gratify the paraphilic craving. Patients suffering obsessive-compulsiveparaphilialogicaldis-orders are often so tortured, absorbed, and compulsively driven by their craving that theordinaryresponsibilitiesofeverydaylife are left completely neglected. The author has noticed that many raptophiles and pedophiles are not continuously obsessive and compulsive; the active periods may be linked to biological variations in serotonin levels, mood, or hormonal variations and bio-social stressors. From these observations, it is fairly reasonable to assume that the loss of impulse control in paraphilic disorders is related to 5-HT2 disturbance in combina-tion with sexual-erotic coding errors that probably occur during critical bio-social times in juvenile life. Impulse control is thoughttobemaintainedbyseveralspecies of serotonin, receptors, but 5-HT2 seems to be a principle player.41 This conclusion is based on recent research that seems to show that 5-HT2 appears critical for the maintenance of impulse control anxiety and obsessive-compulsive kinds of symptomatology. 42 In the author’s unpublished research, sixcasesofchronicpedophiliaweretreated over a 40-week pilot trial with fluvox-amine and clomipramine hydrochloride. Pedophilic craving was evaluated with a modified Y-BOCS. In all cases pedophilic craving was reduced and maintained at the subclinical level. These results will be presented in a future paper. Sexual arousal and orgasm is the key feature of SEAP dynamics in paraphilic disorders. As mentioned in the earlier clinical case of a rapist, in childhood he witnessed numerous brutal and physically violent interactions between his mother and her numerous consort lovers. Thus, in his developmental history, violence, humiliation, and torture of the mother figure became cross coded into the service of arousal and orgasm which is perma-nently fused to sexual and erotic arousal. Whenaskedaboutsexualstimulationunder mild consensual conditions, this patient responded with a chuckle, “that would be boring as hell,” he said, “to do it would be a severe compromise.” Unfortunately, professionals and laymen alike still fail to realize that rapists, pedophiles and all other varieties of paraphiles, tremendously enjoy their aberrant sexual behaviour, and that there is nothing psychological about it. The determining core factor is appetite. In our example of an encoded rape macro, humiliation, brutality, and inflict-ing pain, for the rapist is a kind of sadistic foreplay, what ordinary people can’t imag-ine because they don’t carry an encoded macro for that kind of sexual-erotic ex-pression. The original encoded female, or in some cases, several females, become the model , or template upon which the SEAP is forged. Victims who meet the predeter-mined SEAP criteria are often in jeopardy for their very lives. Rapists and pedophiles literally repli-cate what they have been encoded to do. The codes are so specific that most profes-sionals are baffled by them and muddy the water with all kinds of intrapsychic explanations which, quite literally, have nothingtodowiththesexual-eroticrituals of paraphiles. For example, one particular rapist known to the author typically fled from the scene of his rape to masturbate soloinconcealmentaftertheactualassault. Interestingly,thisindividualoftenwatched his mother’s brutal lovers beat and sodo-mizeher,throughaholeinthewallthathe secretly made. He would masturbate con-cealedfromtheactualplayers.Thisresulted in a pattern whereby, he would attack the victim, but he saved the orgasmic part of the ritual to do in solo masturbation. It is nothing more than experiential encoding or imprinting. SEAP rituals are somewhat different than OCD rituals because they are far less socially stigmatizing. Nobody is going to call the police if they see a man picking garbage, or hoarding paper, but if a man is seen exposing himself genitally, he he may be arrested. In paraphilias, because of the social stigma, the patient tries to hold back the thoughts, behavior and fantasies, but as he does so, craving reaches unbearable levels until loss of impulse control occurs, which probably is generated by pathology in 5-HT2 transmitter dynamics. It is postulated that the obsessive thoughts and rituals of a SEAP have a higher threshold for access compared to those of the OCD Macro because of the social and legal stigma and sanctions involved. The Role of the Serotonin 5-HT2 Receptor FamilyWehavementionedserotoninnumer-ous times in this article. Too much, or too little serotonin seems to cause problems among many species. In humans, it is related to anxiety and OCD disorders, in some species of leeches, depletion stops feeding behavior. 5-HTprojections of all families innervate all major regions of the CNS in man and is especially involved in sexual, and sensorimotor arousal. The 5-HT2 family exerts its effects by increas-ing hydrolysis of phosphoinositol (PI). Of the 14 types of 5-HT serotonin recep-tors, our focus is on 5-HT2. It is fairly well established at this time that 5-HT2 plays a pivotal role in OCD spectrum disorders. We will now explore its role in paraphilialogical disorders with more detail. During the perseveration of the obsessive SEAP thoughts and fantasies accelerate with increasing intensity, and the patient suffers what we call, ‘break-throughs’ (loss of thought or impulse control) that is, associations, thoughts and cognitions become looser, which is sometimes called, cognitive slippage. The patient can’t concentrate clearly, focus be-gins slipping and the obsessive paraphilic thoughts and rituals become stronger and stronger until they take complete control of the patient’s ability to think clearly at all. When this stage of paraphilic access occurs, the rapist, for example, will begin stalking streets, malls, and parks scanning for targets; the pedophile, on the other hand, will frequent arcades, school yards, parks,videostandsanywherehisparticular kindoftargetsaretypicallytobefound.At this stage the paraphile is often desperately trying to talk himself out of the craving, which makes perfect sense, because, this is exactly what most therapists and profes-sionals tell them to do. But it fails as the craving increases higher and higher, until complete paraphilic access occurs. By this point in time, the patient has no voluntary control of anything; and consequences such as jail, mean absolutely nothing. After the paraphilic ritual is complete and orgasm has been achieved, the patient feels guilty because he could not stop what his paraphilic obsession demanded he do. He feels self pity, and is often depressed after-ward, and can’t understand why or how to control the monster within him. These are actual words and phrases recorded by chronicparaphilesoverthousandsofhours of clinical work. The‘breakthroughs’andthecognitive slippage described appears to be related to serotonergic depletion. It is fairly well established in OCD disorders, and the author suspects similar 5-HT2 transmitter dynamicstobeidentifiedinthenearfuture in the neurobiology of paraphil-ialogical disorders. In OCD disorders, this conclusion is also supported by low levels of serotonin metabolite (5 hydroxyindoleacetic acid) found in the spinal fluid of patients with impulse and OCD spectrum disorders. 44 Further, support comes from the author’s unpublished successful applications of SSRIcompoundsonpatientswithchronic pedophilic craving in pilot trials. There seems to be a common link between OCD disorders and what the author has called OCP, which is modulated by 5-HT2 and may also involve cascading effects of other transmitters. Some 200 human neuro transmitters and modulators have been cloned to date and it is not likely thatanysingletransmitterfunctionsalone. These multiple transmitter dynamics will have to be addressed in the future in their relationship to OCP and probably OCD spectrum disorders as well. To date, it has been shown that the selective serotonergic re-uptake inhibitors (SSRI’s)decreaseOCDsymptomotolgy.45–48 In fact, recent meta-analysis studies on OCD may be cautiously applied to OCP. The only effective current treatment apart from neurosurgical procedures is behavior therapy and SSRI.49,50 It doesn’t seem too difficult to design behavioral therapies for ordinary OCD disorders since they don’t carry a legal or social stigma like the paraphilialogical disorders do. Therefore, it is essential to consider the SSRI’s in the long term management of these extremely debilitating disorders. There is convincing evidence that long term administration of SSRI’s may enhance serotonin concentra-tions in the synaptic cleft by desensitizing 5-HT auto-receptors, and thus normalize serotonergic function. SummaryTo summarize, the purpose of this paper is to provide a biomedical model of whatwehavedubbedobsessivecompulsive paraphilia,(OCP).Theauthorhypothesizes thatitisoneofthespectrumofOCDanxi-etydisorders,whichtodatehasnotreceived any clinical attention as a clinical diagnostic disorder. Two major neuroanatomical sites havebeenidentifiedinobsessivecompulsive disorders, which the author hypothesizes may share co-morbidity with the OCD disorders.Thesesitesaretheseptal-hippoc-ampal behavioral inhibition system (BIS) and the prefrontal cortex-basal ganglia-thalamic ‘worry circuit’, both of which are linked by the well described Papez circuit. The cognitive and behavioral activities of the compulsive have been described as being similar in rigidity and sequence to the macro of modern computer programs. Herein, it is postulated a macro for OCP exists in paraphilialogical disorders de-fined as a Sexual-Erotic Arousal Pattern (SEAP). Both OCD macro’s and SEAP macros are believed to result from specific neuromolecular encoding in juvenile life. SEAP codes are believed putatively stored in , or imprinted in the temporal lobe and other anatomical tissue of the brain ready for instant recall or access by the BIS un-der bio-social conditions dictated by the SEAP codes. In conclusion, it is hoped that others will take the seminal suggestions offered, and explore the use of SSRIs and some tri-cyclics, clomipramine in particular, in the long term management of the paraphilic disorders,amongthemostdebilitatingand under-represented biomedical disorders in medical and psychiatric practice today. References1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Washington, DC American Psychiatric Association l994
4 McElroy SL, Philiips KA, Keck PE Jr: Obses-sive Compulsive Spectrum Disorders, J Clin Psychiat Suppl. l994; 55: 43. 5 Rasmussen SA, Tsuang MT: Clinical Charac-teristics and Family History in DSM-III Ob-sessive-Compulsive Disorders, Am J Psychiat l986; l43: 3l6-322
10.McElroySL,PhilipsKA,KeckPEJr:Obsessive CompulsiveSpectrumDisorder JClinPsychiat Suppl, l994; 55: 42 11.Baxter LR: Positron Emission Tomography Studies of Cerebral Glucose Metabolism in ObsessiveCompulsiveDisorder JClinPsychiat Suppl, l994; 55: 58 14.Grey JA: The Neurobiology of Anxiety, 1st Edition, New York, Oxford University Press, l982: 11. 13.Grey JA: The Neurobiology of Anxiety, 1st Edition, New York, NY: Oxford University Press, l982: 440. 14.Rasmussen S A: OCD: A Review of its Pheno-monology and its Infuence on Diagnosis. Audio Digest Psychiatry, l995; 21, 21: Vol 1 15.Lorenz K: King Solomon’s Ring, New York. Thomas Cromwell. l952. 16.Lorenz K: Aggression, Harcourt Brace World, New York. l963. 17.Tinbergen N: Early Childhood Autism: an Ethological Approach. Compar Ethol Suppl, l972; l0: 9. 18.MontarolaPG,KandelER,Schacher,S:Long-term Heterosynaptic Inhibition in Aplysia. Nature 1988; 333: l7l-l74. 19.Kuno M: The Synapse: Function, Plasticity and Neurotropism; New York. Oxford Uni-versity Press, l995; 38. 20.Yeh Shih-Rung, Fricke RA, Edwards DH: Science, l996; 27l: 366-369. 21.SingerW:DevelopmentandPlasticityofCor-tical Processing Architectures, Science, l995; 270: l58-l64. 22.Bremer JD: Am J Psychiat 6: l995. 23.Shepard, G: Neurobiology; New York. Oxford University Press, l994. 24.Wilson JD, Braunwald E, Isselbacker KJ, Ptersdorf RG, Martin JB, Fauci AS, Root RK, Eds. Harrison’s Principles of Internal Medicine, l2th Ed. New York. McGraw-Hill, 1991: 201. 25.Grey JA: The Neurobiology of Anxiety, First Edition, New York. Oxford University Press. l982: l2. 26.Baxter LR: Positron Emission Tomography Studies of Cerebral Glucose Metabolism in ObsessiveCompulsiveDisorder. JClinPsychiat Suppl, l994; 55: 54-59. 27.Papez J: A Proposed Mechanism of Emotion Arch Neurol Psychiat, l938; 725-743. 28.Grey JA: The Neurobiology of Anxiety, 1st Edition, New York. Oxford University Press; l982: 294. 29.Grey JA: The Neuropsychology of Anxiety, 1st Edition, New York, NY: Oxford University; 1982; 459 - 461. 30.Grey JA, The Neuropsychology of Anxiety, 1st Edition, New York. Oxford University; 1982; 92. 31.Baxter LR: Positron Emission Tomography Studies of Cerebral Glucose Metabolism in Obsessive Compulsive Disorder. J Clin Psy-chiat, Suppl. 1994; 55: 58. 32.Baxter, LR: Positron Emission Tomography Studies of Cerebral Glucose Metabolism in Obsessive Compulsive Disorder. J Clin Psy-chiatry Suppl. 1994, 55: 57. 33.Kaplan HI, Freedman AM, Adock BJ, Com-prehensive Textbook of Psychiatry. 3rd Edi-tion. Vol 2, Williams and Wilkins. Baltimore London 1980 Pg. 57 34.Grey JA, The Neuropsychology of Anxiety, 1st Edition. New York, NY: Oxford University Press; 1982 Pg. 453 35.Grey JA, The Neuropsychology of Anxiety, First Edition. New York, NY: Oxford University Press; 1982 Pg. 436 36.Eison MS, Stark AD, Ellison G: Opposed Ef-fectsofLocusCoeruleusandSubstantiaNigra Lesions on Social Behavior in Rat Colonies. Pharmacol Biochem Behav, 1977; 7: 87-90. 37.Grey JA, The Neuropsychology of Anxiety, 1st Edition. New York. Oxford University Press; 1982; 436. 38.Baxter LR: Positron Emission Tomography Studies of Cerebral Glucose Metabolism in ObsessiveCompulsiveDisorder. JClinPsychiat Suppl, 1994; 55: 58 39.Grey JA: The Neuropsychology of Anxiety, 1st Edition. New York. Oxford University Press; 1982: 454. 40.Kate RJ: Neurobiology of Obsessive-Compulsive Disorder -A Serotonergic Basis of Freudian Repression. Neurosci Biobeh Rev, 1991;15: 375-381. 41.Stein DJ, Hollander E, Anthony DT et al: Se-rotonergic Medication for Sexual Obsessions, Sexual Additions, and Paraphilias, J Clin, Psychiat 1992; 53: 267 - 271. 42.Relapse Prevention, Brandon, Vermont, Safer Society Press. 43.Gibbs WW: Seeking the Criminal Element. Sci Amer, 1995; 3: 100 - 107 44.Fountaine R, Chouinard G: Fluvoxamine in ObsessiveCompulsiveDisorder. PsychiatAnn. 1989; 19: 92-96. 45.KafkaMP:Successfultreatmentofparaphiliac coercive disorder (A Rapist) with fluoxetine hydrochloride. Br J Psychiat 1991; 158: 844- 847. 46.Emmanuel NP, Lydiard RB, Ballenger JC: Fluoxetine Treatment of Voyeurism (Letter) Am J Psychiat, 1991; 148 - 950 47.Bianchi MD: Fluoxetine Treatment of Exhi-bitionism (Letter) Am J Psychiat, 1990; 147: 1089-1090 48.Goodman WK, Price LH, Delgado PL, et al: Specificity of Serotonin Reuptake Inhibitors in the Treatment of Obsessive-compulsive Disorders: Comparison of Fluvoxamine and Desipramine. Arch Gen Psychiat, 1990; 45: 577-585. 49.Greist JH, Jefferson JW, Kobak K, et al: Ef-ficacyandTolerabilityofSerotoninTtransport Inhibitors in Obsessive-compulsive Disorder: A meta-analysis. Arch Gen. Psychiat, 1995; 52: 53-60. 50.Murphy DL, Pigott TA: A Comparative Ex-amination of a Role for Serotonin in Obses-sive-Compulsive Disorders, Panic Disorder and Anxiety. J Clin Psychiat Suppl. 1990; 51: 53-58. 51.Leonard BE: The Comparative Pharmacology of New Antidepressants. J Clin Psychiat Suppl, 1993; 54: 3-15. 52.Christensen H, Hadzi-Pavlovic D, Andrews G, et al: Behavior Therapy and Tricyclic Medication in the Treatment of Obsessive-Compulsive Disorder: A Quantitative Review. J Consult Clin Psychol, 1987; 55: 707-711. |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)