 |

|
|
|
|
 Back to 1996 4th Quarter Table of Contents
Back to 1996 4th Quarter Table of Contents
The results of this study indicate that proper amalgam removal and, in some cases, removal of all the other metals and replacement with biocompatible composites can eliminate or reduce 80% of the classic symptoms of chronic mercury poisoning. These results also show that the strength of an individual’sserum-globulin reaction,to many metals used in dentistry, especially the five metals present in amalgam, has important implications for recovery. IntroductionIt has been documented that mercury escapes from amalgam fillings and adversely affects health.1-3 Many clinical experiments have also demonstrated that symptoms associated with mercury poisoning greatly decrease when amalgam fillings are removed and replaced by less toxic materials–for example, composite materials. 4–8 Thisstudydiffersfromsimilarclinical studies in demonstrating the correlation between the patient’s serum-globulin reaction to dental metals and the patient’s response after amalgam fillings (and other metals) are replaced with composite materials found to be biocompatible with the individual patient. One hundred eighteen patients participated in this study, consisting of 97 women and 21 men ranging in age from 18 to 73 years. The average age of participants was 45 years. Before treatment began in 1990-91, a blood serum test was performed on each patient in order to determine which dental materials caused minimal reactions in the individual. This 1. Torvet 1A. 3400 Hillerød. Denmark. serum analysis incorporated globulin reactions for metals. Scientific research by Pleva, Clarkson, Masi and many others has proven that metals are essential for normal human functioning. However, certain metals are poisonous, even in extremely small quantities, and serve no biological function. Heavy metals, including mercury and cadmium, are in this category.9–11 Other metals, for example, copper, zinc and selenium,arenecessaryinminutequantities, but are toxic in large quantities. Products ofcorrosionandmetalswhichreactchemically with proteins or methyl groups are extremely poisonous.12 Removing all dental metals, thereby removing a constant and probably excessive sourceofexposuretometals,couldobviously have a positive impact on the patient. Individuals react differently to many metals, as demonstrated by the blood serum test. This suggests that individuals will show varying degrees of improvement when exposure to these metals ceases. Method and ResultThe 118 patients involved in this study completed a survey discussing 38 classic symptoms of chronic mercury poisoning.Beforeremovalofamalgam(andin somecases,additionalmetals)eachpatient underwent a blood serum test of their globulinreactionto34differentmetalsand assorteddentalmaterials.Thepatientsthen had all amalgam fillings removed. Some patients also elected to have other metal and porcelain dental work removed. Symptoms Before Amalgam RemovalThe survey covered 38 symptoms and complaints common to chronic mercury poisoning, as found in related literature. Participatinginthesurveywere118patients who have been with my clinic since 1984. The following symptoms and complaints were common–before amalgam removal– to more than 50% of the par
Priortoamalgamremoval,allpatients hadanaverageof17.4ofthe38symptoms and complaints listed in the study. The 58 patients who reacted strongly to many metals had on average no more symptoms and complaints than the 60 patients who demonstrated milder total reaction to metals. Blood Serum Globulin ReactionAll patients had a blood test taken at an authorized laboratory. The separated blood serum was frozen and sent via SAS Cargo to the Diagnostic Center’s laboratory in Colorado Springs, Colorado, USA. Thislaboratory,underthedirectionofHal Huggins DDS, MS, is state approved and highly reputable.13 Another laboratory in Colorado Springs, under the direction of W.J. Clifford, MS, member of IAOMT (International Academy of Oral Medicine and Toxicology), performed the same serum analysis.14 The test performed is described in medical literature as a precipitin test. The test determines the quantity of globulins (IgA, IgG and IgM) formed when the patient’s blood serum comes in contact Table 1. Precipitin Globulin Test for Dental Materials and other Metals. Strong Reaction Moderate Reaction Reaction on “Amalgam-metals”
withthemetals,componentsandcorrosion products in many dental materials. The globulins are measured photometrically and the results indicate the relative serum reaction of individual patients. Besides the dental materials, the blood serum test applies to 34 additional metals. Participants responded positively to 32 of these metals. The distribution of patient’s response is shown in Table 1. Serum tests of patients showed that 98% reacted to some of the most popular composite materials. About 75 participants reacted to aluminium, which is present in many dental filling materials. Because aluminium is present in all glass ionomers, all patients who react to aluminium will react to this material. Some sufficiently strong composite dental materials, for example, Posterior II and Conquest, do not contain aluminium. These are composed of substances and metals to which most patients react mildly. Metals Used in DentistryA tremendous variety of metals are used in dentistry. A gold crown normally consists of gold and platinum and may contain many different metals, especially in the case of a “discount crown,” where silver, copper, palladium, tin, indium and/or molybdenum are substituted for the expensive metals. The metal hardware under porcelain crowns frequently contains gold, palladium, silver, platinum, tin, indium, gallium and copper. Wires for regulating teeth and bands placed around teeth are composed of nickel, chromium, molybdenum and silicon. Denturesmadeofmetal,so-called unitors, are usually made of cobalt, chromium, molybdenum, silicon, titanium and sometimes nickel. Many patients demonstrate globulin reactions to these metals, as indicated by the blood serum test. Participants reacted to a range of three to 19 metals, the average participant reacting to 10 metals. The metalreactionswerecalculatedwithvalues ranging from 1 to 9 for each metal, 9 being the strongest reaction. The average combined reactions to all metals totaled 40 points, ranging from 6 to 108 points. When the 5 amalgam metals (mercury, copper, silver, tin and zinc) are considered exclusively,theaveragereactionis20points ranging from 2 to 45 points. The known potency of the material must be taken into consideration when comparing these reactions. For example, beryllium and mercury are known to cause adverse reactions with extremely small doses. Other metals like copper and aluminium may cause a relatively higher reactionas measured inpoint,without being more dangerous.However,in this study this issue is immaterial because for each patient we compare the total of reactions to all metal/amalgammetal with their symptoms before and after removal of metals. We compared the change in the symptoms of participants who reacted strongly to amalgam metals with those of participants who reacted mildly to amalgam metals, and the same procedure was followed for those who had astrong or mild reaction to other metals. All amalgam fillings were replaced in all participants. Two thousand six hundred amalgam areas were removed, averaging 22 areas per patient. Twenty-nine patients had all other metals replaced, especially gold/porcelain. This group had 128 gold surfaces, average 4.4 per patient. The replacement of fillings took place according to methods recommended by Huggins, Colorado Springs, USA. His recommendations include:
4.Carbon tablet ingestion before and after 31% symptoms eliminated 21% symptoms unchanged 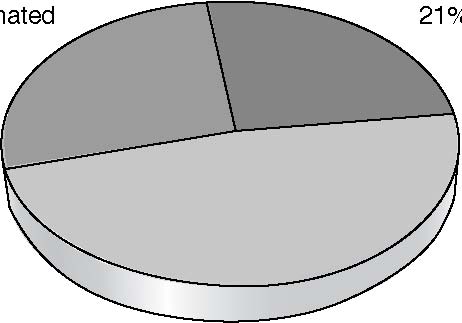 48% symptoms reduced Figure 1. Change in Symptoms in Percent of the Whole Group after Proper Amalgam Removal each treatment. 5.One drink of alcohol immediately before treatment.
All questions arising during treatment were addressed and the best results are obtained when both doctor and patient follow these methods. Results After Proper Amalgam RemovalAfter amalgam removal, 79 participants had no amalgam or metals remaining. Thirty-nine had no visible amalgam, having elected to retain one or more gold or porcelain crowns, under which amalgam may be present. One to four years after removal, all patients responded to the same survey as previously noted, inquiring whether the 38 symptoms and complaints had improved, disappeared, or remained unchanged. The results of this survey indicate that for the average participant regarding the 17 symptoms, 8.2 were reduced, 5.1 were eliminated, and 3.7 were unchanged. In other words, 48% of symptoms were reduced, 31% were eliminated, and 21% were unchanged (Figure 1). In total, 79% of the symptoms and complaints were reduced or eliminated after amalgam removal. In over 90% of responses, the following symptoms were reduced or eliminated: tender teeth; bad breath; metallic taste; diarrhea; leg cramps; frequent infections. In over 80% of responses, the following symptoms were reduced or eliminated: bleeding gums; blisters and sores; throat pains; nasal congestion; nasal discharge; irrational fear; headache, migraine, irritability, insomnia, dizziness, and muscle tremors. The study depicted in Figure 2 indicates that patients with mild reactions to metals are more likely to have fewer or no symptoms than those patients with strong reactions. This difference is more pronounced when comparing patient’s reactions to 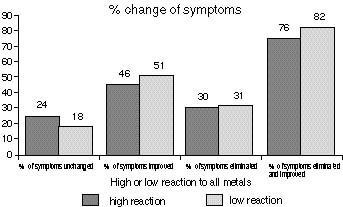 Figure 2. 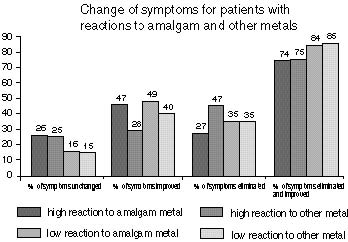 Figure 3. the five amalgam metals (mercury, silver, improvement in the following symptoms: copper, tin and zinc). Patients with strong allergies; skin problems; tender teeth; nasal amalgam metal reaction showed reduction discharge; constipation; fatigue; insomnia; or elimination of 74% of symptoms and muscle fatigue; muscle tremors; sciatic pain; complaints, whereas patients with mild joint pain; cold hands and feet, and frequent amalgam metal reaction showed reduction infections.The group with strong metal reacor elimination of 84% (Figure 3). tion showed greater than 10% improvement In Table 2 we see the group with mild in the following symptoms: blisters and sores; metal reaction showed greater than 10% digestive pain; heart problems. Table 2. Changes in Individual Symptoms and Complaints Following Amalgam Removal. No. of symptoms before amalgam removal.No. of symptoms reduced after amalgam removal. No. of symptoms eliminated after amalgam removal. % of symptoms reduced or eliminated for those that had: low metal reaction. high metal reaction. Symptoms/complaints
DiscussionFor years, science has demonstrated that mercury found in the body comes primarily from amalgam fillings.15 It is also widely understood that many of the metals used in dentistry are toxic or hazardous.16 Innumerable scientific experiments on animals and humans have demonstrated that mercury from amalgam is hazardous to cells and functions of organs. Specifically, mercury affects the immune system;17 the kidneys;18 mouth and colon bacteria;19 the reproductive system;20 and the central nervous system.21 Many clinicians have demonstrated over the course of the past century that removal of amalgam fillings and gold/porcelain fillings improves an extensive array of symptoms, complaints and diseases which have been otherwise unsuccessfully treated. Professor Fredrik Berglund’s book, which appeared in 1995, surveyed the literature on this subject and collected the case histories of 150 patients whose diseases, symptoms or complaints were eliminated or reduced after removal of amalgam and other metals.22 Metal-Free Dentistry Is Possible TodayDental use of metals is no longer necessary thanks to good composites and especially to the new PCDMA-based, shock-absorbing and extremely durable composites.23–25 Laminate fortified composites with characteristics very similar to natural tooth material are now used for crowns and bridges.26,27 These materials are tested for biocompatibility with the individual patient. This study demonstrates the positive results of removing amalgam fillings and other metals from patients who suffer from an extensive array of symptoms which they have not otherwise been able to treat successfully.Obviously,some participants may anticipate improvement, which in itself may result in improvement. This placebo effect results in 20-25% improvement at best and disappears gradually over time. It generally takes six to 12 months or longer for symptoms to be eliminated or reduced. Patients completed surveys one year after treatment, and in some cases, again four years later, to take into account the slow therapeutic effects of amalgam removal. Metal DepositsPatients generally improve gradually as years pass after amalgam removal. This correlates with the fact that large deposits are continuously found in the tissues of the body and are slowly eliminated. An active detoxification treatment could accelerate the improvement. The patients with a strong reaction to amalgam metals did not recover as favorably as those with mild reactions. Metal deposits in tissues and organs may be present for years in different degrees in these two groups of patients. PyorrhoeaPeriodontal diseases is very common. Forty-two percent of the participants in this study had bleeding gums and 46% had tender teeth, before amalgam and metal removal. It is commonly believed that bleeding gums and tender teeth are the early symptoms of pyorrhoea and are caused by plaque and microorganisms on teeth and in teeth sockets. However, the results of this study indicate that metals and specially amalgam metals are the actual cause.28 In this study, 88% of the incidence of bleeding gums was reduced or eliminated, and 91% of the incidence of tender teeth was reduced or eliminated Digestive ProblemsDigestive problems were very common among participants.They can be caused by many factors, but amalgam removal demonstrates a strong positive effect on these problems. The mercury released from the amalgam fillings combines with the saliva, forming extremely poisonous methyl-mercury in the mouth,stomach and colon.The composition of digestive bacteria is changed as a result, and mostly mercury-resistant bacteria survive.Thus,manybacteriaessentialto healthy digestion are destroyed. A new study indicates that people with amalgam fillings have many more strains of penicillin-resistant bacteria than those without amalgam fillings.19 The results after amalgam removal are as follows. (Expressed as the percent of patients experiencing reduction or elimination of symptoms) Pressure and air in stomach (bloating)74%
Problems with the central nervous system are also very common.(Table 2) Both recent and earlier studies demonstrate that mercury escaping from amalgam fillings, especially as mercury vapor, can harm the central nervous system. Alzheimer’s disease is a primary example of this.21 The results after amalgam removal are as follows: (Expressed as the percent of patients experiencing reduction or elimination of symptoms) Headache 85% Migraine 81% Poor concentration 71% Poor memory 70% Irrational fear 88% Irritability 80% Dizziness 89% Muscle tremors 79% Leg cramps 90% Immune SystemThe immune system is often debilitated by mercury.17 Symptoms frequently include fatigue and frequent infections. These symptoms are significantly reduced or eliminated, as demonstrated by the following results. (Expressed as the percent of patients experiencing reduction or
Experiments with sheep and monkeys with implanted amalgam fillings demonstrate reduced kidney function.30 Patients in this study also experienced similar improvements.(Expressed as the percent of patients experiencing reduction or elimination of symptoms) 25% of participants had urinary system disorders prior to amalgam removal. 52% of these patients experienced reduced symptoms after amalgam removal. 17% eliminated urinary system disorders after amalgam removal. ConclusionMany symptoms commonly associated with mercury intoxication can be related to harmful effects from metals used in dentistry. About 16,500 observations were gathered during the prolonged study of these 118 patients; these data indicate that about 80% of the symptoms and complaints were eliminated or reduced one to four years after removal of dental metals, especially amalgam metals (mercury, silver, copper, tin and zinc) and proper replacement with biocompatible plastic. This study confirms other classic and scientific results,30,31 and suggests that dentists should avoid the use of metals because of the reactions they clearly cause in many patients. The greatest positive reactions are shown by the group with the mildest blood serum-globulin test reaction for the amalgam metals. This suggests that the determining factor for the degree and rate of recovery is dependent on the patient’s individual tolerance and degree of reaction to certain metals. References
388. 10.ClarksonTW,HurshJB,SagerPR&Syversen TLM: In eds. Clarkson TW, Friberg L, Norberg G F, & Sager PR: Mercury in Biological Monitoring of Toxic Metals, NewYork,Plenum, 1988; 199-246. 11. Masi J V: Corrosion of amalgams in restorative materials: the problem and the promise. In eds. Friberg L, Schrauzer GN: Status Quo and Perspectives of Amalgam and other Dental Materials, Stuttgart. Thieme-Verlag. 1995. In press. 12.Gross MJ & Harrison JA: Some electrochemical features of the in vivo corrosion of dental amalgams. J Appl. Electrochem. 1989; 19: 301-310. 13.Huggins H: Medical and Legal Implications of Components of Dental Materials. P.O. Box 2589 Colorado Springs, CO, 80901. U.S.A. 1989. 14.Clifford WJ:Materials reactivity testing Background, basis and procedures for the immunological evaluation of systemic sensitization to components, which emanate from biomaterials. P.O. Box 17597 Colorado Springs, CO, 80935. U.S.A. 1987–1989. 15.FribergL,ed: Inorganicmercury. Environmental Health Criteria 118, Geneva World Health Organization. 1991. 16.StörtebeckerP:MercuryPoisoningfromdental amalgam. Störtebecker Fdn Res. Orlando, FL. Bioprobe. 1985; 138,149,151-54. 17.Hultman P, Johansson U, Turley SJ, Linh U, Enestrøm S & Pollard KM: Adverse immunological effects and autoimmunity induced by dental amalgam and alloy in mice FASEB J, 1994; 8: 1183-1190. 18.Zalups RK: Autometallographic localization of inorganic mercury in kidneys of rats: Effect of unilateral nephrectomy and compensatory renal growth. Exp Mol Pathol. 1991; 54: 10-21. 19.Summers AO, Wireman J, Vimy MJ, Lorscheider F L, Marshall B, Levy S B, Bennett, S & Billard L: Mercury released from dental “silver”fillings provokes an increase in mercury and antibiotic-resistant bacteria in oral and intestinalflorasofprimates. AntimicrobAgents Chemother, 1993; 37: 825-834. 20.Rowland AS, Baird DD,Weinberg CR, Shore DL, Shy C M & Wilcox AJ: The effect of occupational exposure to mercury vapour on the fertility of female dental assistants. Occup Environ Med. 1994; 51: 28-34. 21.Lorscheider FL,Vimy MJ,Pendergrass JC, & Haley BE: Toxicity of ionic mercury and elemental mercury vapor on brain neuronal proteinmetabolism.12th International Neurotoxicologyconference, HotSprings, AR, 10/31: 1994. Neurotoxicol 1994; 15: 955. 22.Berglund,F. 150 years of dental amalgam.1995; Orlando, FL. Bio-Probe Inc. 23. Waknine S et al:Direct/indirect commercial composites characterization on strength shrinkage and wear. Acapulco, IADR, 1991: 1722. 24.WaknineS: Conquest DFC: ANovel Universal Dental Composite restorative System. Journal of Aesthetic Dentistry Update. 1991; 2: 70-79. 25.WaknineS, Goldberg AJ, MeullerHJ,Legeros J, Prasad A, & Schulman A: Fracture Toughness of a New Semi-Crystalline Resin. Paper 1660, J. Dent Res. 1992. Amer Assoc Dent Res. 1992; 3: Boston, MA. 26.Ogolnick R, Picard B & Denry I; Cahiers de Biomateréiaux Dentinaires. No. 2 Materiaux Organiques, Paris. Masson. 1992. 27.Waknine S, et al: Fracture toughness of a new semi-crystalline dental resin. MDR 1660 Chicago, IL 1992. 28.Siblerud RL: The relationship between mercury from dental amalgam and oral health. Annals of Dentistry. 1990; 49: 6-10. 29.Hahn LJ, Kloiber R, Leininger RW, Vimy, MJ, & Lorscheider, FL: Whole-body imaging of the distribution of mercury released from dental fillings into monkey tissues. FASEB J, 1990; 4: 3256-3260. 30.Lorscheider F L, Vimy MJ, Summers AO: Mercury exposure from “silver” tooth fillings: 31.Friberg LT, Schrauzer GN: Status Quo and emerging evidence questions a traditional Perspectives of Amalgam and other dental Ma-dental paradigm. A review. FASEB J, 1995; terials. International Symposium Proceedings, 9: 504-508. New York. Verlag Stuttgart. Georg Thieme. Plan to join us for theNUTRITIONAL MEDICINE TODAY 26thAnnual International ConferenceApril 18-20, 1997, Toronto, Canada Royal York HotelAbram Hoffer, MD, PhD Victoria, CanadaMikhael Adams, BSc, ND Toronto, CanadaArnaldo Velloso Da Costa, MD Sao Paulo, Brazil David Horrobin, D Phil, BM, BCh Nova Scotia, Canada Oslim Malina, MD Curitiba, BrazilE. Vogelaar, PhD NetherlandsGert Shuitemaker, PhD NetherlandsCharles Simone, MD New JerseySherry Rogers, MD New York, USAJohn Smythies, PhD California For more information please contactThe International Society forOrthomolecular medicine 16 Florence Avenue, Toronto, Ontario, Canada M2N 1E9Tel: (416) 733-2117 Fax: (416) 733-2352 E-mail: centre@orthomed.org http://www.orthomed.org | |||||

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)