 |

|
|
|
|
 Back to 1996 4th Quarter Table of Contents
Back to 1996 4th Quarter Table of Contents
An article in the New England Journal of Medicine from 1988 drew the attention to a scant discerned problem: neuropsychiatric disorders due to vitamin B12 (cobalamin) deficiency occured in patients, mainly elderly, who didn’t present with hematological deviations.1 After administration of vitamin B12, the symptoms disappeared in practically all patients. The research demonstrated that in daily practice a deficiency of vitamin B12 is often not recognized as the cause of severe and frequently occuring psychiatric disorders. Advanced research confirmed these results.2 Other research points out the danger of undiagnosed vitamin B12 deficiency, especially in pernicious anaemia. B12 Status and Pernicious AnemiaPernicious anemia is an autoimmune disease with the principle characteristic being that the stomach is not able to produce intrinsic factor necessary for adequate resorption of vitamin B12 from food. The disease shows a megaloblastic blood picture as a result of a chronic lack of vitamin B12. Suprisingly,there search shows on lyaslight connection between low vitamin B12 status and pernicious anaemia.3 Yet vitamin B12 blood levels are important for the diagnosis of pernicious anaemia. For this reason pernicious anaemia is often missed. Furthermore, a correct diagnosis is hindered by therathera specificity of vitamin B12 deficiency, and such a deficiency manifesting itself over the long term. Also the general opinion that storage of this vitamin in the human body is sufficient to supply it for three to six years does not help in diagnosing pernicious anemia adequately. The first symptoms of acobalaminde 1. Ortho Institute, P.O. Box 82, 7080 AB Gendringen, The Netherlands. ficiencyarepalenessandfatigue.Ingeneral, deficiency is diagnosed on the observation of enlarged red blood cells (macrocytosis). However this symptom cannot be distiguished from folate deficiency. The general opinion is that distinction usually only manifests after several years, when neuropsychiatric symptoms come forward: tingling hands and/or feet (always symmetrical), boredom, fatigue and lethargy, shortness of breath, palpitations, sore mouth with a thick, often painful tongue. Frequently a pale complexion with soft yellow discoloration (because of a deteriorated liver function) is seen. Irritability, loss of memory,mild depression and mood swings can also be observed. B12 Deficiency and Alzheimer’s DiseaseNew methods to assess vitamin B12 status show that vitamin B12 deficiency occurs much more often than was previously assumed.4 Assessment of the methylmalonic acid level is a precise method to determine possible existence of vitamin B12 deficiency, if necessary supported by assessment of homocystein and cystathionin. When these assessments are performed in elderly people, high percentages are often found, which indicates the existence of deficiencies of the vitamins cobalamin, folic acid and pyridoxal phosphate(vitamin B6) in the elderly.5 Ten percent of all people between 65 and 75 years old, 20% of those between 75 and 85 years old and 30% of all those over 85 years old suffer from some sort of dementia.6 The literature provides extended information on the deteriorated vitamin B12 status in patients with senile dementia of the Alzheimer type (SDAT). Van Tiggelen described subnormal levels of vitamin B12 in the cerebrospinal fluid of SDAT patients, in spite of normal serum levels.5,7 Later others described B12 anomaly in SDAT patients.8,9 To clarify connections mentioned above one should first gain some insight into the reactions of methylation (Figure 1)10 MethylationIn the body cobalamin is active in two forms. As adenosylcobalamin, a cofactor of the enzyme methylmalonyl-CoA-mutase, or as methylcobalamin, a cofactor of the enzyme methionine synthase. The first form (adenosylcobalamin) is involved in conversion of methylmalonyl-CoA (MM-CoA) into succinyl-CoA. In case of shortage of vitamin B12 this conversion takes place insufficiently and a different conversion takes place of MM-CoA, namely in methylmalonic acid (MMA). A raised MMA-level can serve as an exclusive rate of vitamin B12 deficiency. This conversion is particularly important in the brain and is known as the propionate metabolism.11,12 These condform of vitamin B12 (methylcobalamin) is coenzyme of methionine-synthase. This is an important enzyme in thereactionwhichtransfersamethylgroup from 5-methyltetrahydrofolate (5-MTHF) to homocysteine, forming methionine. This reaction is the key reaction of the so called methylation, a series of reactions in the body transferring methyl groups. In these reactions S-adenosyl methionine (SAM) is used as methyl donor by methyl-transfer as eenzymes.SAM is synthesized from methionine.11,12 Methylation is Part of Many ProcessesMethyltransferases take part in a large number of body processes,including regulation of protein structure, regulation of DNA expression, production of phospholipids, and production of certain hormones and neurotransmitters.10 There are also indications that methylation of phospholipids is the common mechanism of receptor signalling across cell membrane.13 Methyltransferases transfer a methyl group away from S-adenosylmethionine (SAM) forming S-adenosyl-homocystein (SAH). SAH is a strongly competitive inhibitor of methyltransferases and accumulation of SAH in the cell will inhibit methylation reactions. The ratio between these two compounds is called the methylation ratio. A low ratio indicates inhibition of methylation. SAH is broken down by S-adenosyl-homocysteinhydrolase into homocysteine and adenosine. Adenosine is rapidly metabolised into, for example, inosine. Homocysteine has three elimination path-ways: remethylation to methionine (the main elimination route), breakdown to cystathionine or excretion from the cell. Remethylation in the BrainRemethylation of homocysteine is possible in two ways. The first is by way of the above mentioned enzyme methionine synthase, but remethylation can also take place by way of the enzyme betaine meth-yltransfersase. This enzyme is present in only a few organs,such as liver and kidneys Figure 1. The Methylation Process 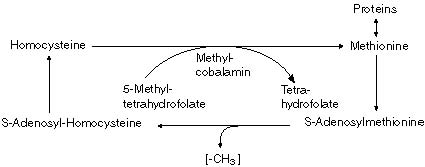 191 Journal of Orthomolecular Medicine Vol. 11, No. 4, 1996 and is not present in the brains.In this case methylation reactions depend totally on functioning of methionine synthase.10 When both remethylation pathways fail, homocysteine is converted with difficulty into cystathionine , and cysteine because the regulating enzyme is activated by high levels of SAM, and these are lacking.ConsequentlySAHandhomocysteine accumulate, the ratio between SAM and SAH (methylation ratio) is low and methylation is inhibited.10 The brain is capable of remethylation of homocysteine exclusively by way of methionine synthase and in case of disfunctioning methionine synthase enzyme is totally dependent on plasma methionine supply, derived from food or from organs such as the liver,which has the disposal of an alternative synthesis pathway. If this supply also fails, clinical symptoms manifest. Neuropathy Caused by B12 DeficiencyNeuropathy as a complication of cobalamin deficiency is characterized by demyelinisation of the posterolateral nerves of the spine. At first it was thought to be due to a disturbance of the enzyme methylmalon-CoA-mutase. Shortage of adenosylcobalamin may inhibit the enzyme, which may result in production of abnormal fatty acids. Incorporation of these defective fatty acids in myelin may lead to demyelination.14 Recent evidence however points to a mechanism by way of the enzyme methionine synthase by methylcobalamin. The most important proof of this is derived from experiments with nitrogen oxides. Nitrogen oxides are strong inhibitors of the enzyme methionine synthase. They inactivate methylcobalamin by oxidation of monovalent cobalt groups to cobalt oxide,which then forms biological inactive cobalaminanalogues.Exposuretonitrogen oxides (also in anaesthesia) results in neuropathy in humans, primates, fruitbats and pigs.15 In cerebrospinal fluid and neural tissueoftheseanimalsextremelylowratios of SAM to SAH are found after exposure to nitrogen oxides. Adequate supply of methionine appears to be able to prevent neuropathyatleastpartly.15 Theadditionof S-adenosylmethionine itself appears in several studies to have many beneficial effects on the central nervous system, especially on the monoamine neurotransmitter metabolism and receptor systems. Provision of these methyl donors is responsible for there myelination observed in patients with inborn disorders of folic acid metabolism and methylation.16 Affected Liver is an Extra Risk FactorIn patients with affected liver function, such as in alcoholics, chronic phenytoin users and patients exposed to hepatotoxic chemicals with neurotoxic potential, abnormally low levels of cobalamin are found in cerebrospinal fluid.7,17 This could be indicative of an abnormal conversion of neurologically active cobalamin by the affected liver, for example by changed activity of microsomal liver enzymes.18-20 In patients with predominantly neurological symptoms of cobalamin deficiency, higher serum levels of cobalamin analogues are found than in patients with hematological symptoms.21 This finding is supported by data derived from studies of alcoholics.22 Interaction with Thiamine MetabolismIt is possible that functional vitamin B12 deficiency blocks resorption, transport and biological activity of thiamine. In particular, methylcobalamin deficiency could induce reduction of the intestinal alkaline phosphatase level, blocking intestinal resorption and possibly alsobiological activation of thiamin.23,24 Deficiency of biological active thiamine in the brains is connected with a range of neurological diseases, as is known from brain research in chronic alcoholics. Folic AcidFolate deficiency is common in elderly. Research among 1250 randomly selected 192 Cobalamin Deficiency, Methylation and Neurological Disorders elderly persons showed that 8% had low serum folate levels.25 Alcoholics, too, run a higher risk of folate deficiency because alcohol specifically affects the formation of tetrahydrofolate. At first,effects of folate deficiency are indistinguishable from vitamin B12 deficiency.Differentiation between these deficiencies is possible only after a long period,when vitamin B12 deficiency is visible by degeneration of nerve tissue. The biologically active form of folic acid in the body is 5-methyltetrafolate (5-MTHF), mentioned before as a methyl donor for the enzymemethioninesynthase, that converts homocysteine to methionine. The body, as mentioned, has at its disposal alternative supply routes for methylgroups in case of insufficient supply of folic acid. But in longstanding folate deficiency these protective mechanisms, too, may fail and result in neurological disorders. Folic acid can act in methylation reactions in other ways. Several interactions are documented between vitamin B12 and folic acid, which suppose that folic acid,orrather5-MTHF, plays a part in the conversion of cobalamin to methylcobalamin.26 This theory is supported by clinical observations of patients with aneuropsychiatric syndromes which are responsive to folate. In research in elderly patients with depression associated with mild dementia, 5-MTHF supplements remedied symptoms in 45% of cases, compared to 29% in the control group treated with trazodone.27 In epidemiologic research psychiatric disorders such as depression, mania, schizophrenia, personality disorders and dementia are also connected with folate status. The main relationship was found with depression and schizophrenia.25 This may be due to the fact that absorption of folic acid from the gastrointestinal tract is inhibited specifically by antidepressants and anti-epileptics. ConclusionVitamin B12 deficiency is often not recognized as the root of neurological syndromes and can occur without reduced serum level or hematological deviations. Assessment of the methylmalonic acid level is a specific and reliable method to determine vitamin B12 status. Elderly people often appear to have abnormal methyl malonic acid levels, which indicates disturbed methylation. Senile Alzheimer’s dementia, too, is often accompanied by an affected B12 status. The brain has available,inconstrast to organs such as the liver, only one method to remethylate homocysteine to methionine. However B12 deficiency inhibits the enzyme responsible for this conversion, and the brain, therefore, becomes totally dependent on supply of methionine in the blood.When this supply fails,neuropathy, among other things, may develop. Folic acid as methyl donor is an important factor in methylation and also in converting vitamin B12 into a biological active form. A complicating factor when the liver is affected by alcohol or toxic substances. As a consequence vitamin B12 is probably converted abnormally,through which biological inactive cobalamin analogues enter the bloodstream. Disturbance of vitamin B1 metabolism may also contribute to development of neurological symptoms in vitamin B12 deficiency. References1. Lindenbaum J, Healton EB, Savage DG, et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. New England J of Med, 1988; 318: 1720-1728. 2. Stabler SP, Allen RH, Savage DG, Linden-baum J. Clinical spectrum and diagnosis of cobalamin deficiency. Blood, 1990; 76:871-881.
Jul;60(1):147] [see comments]. Am J Clin Nutr, 1993; 58:468-476.
10.Weir DG, Scott JM. The biochemical basis of the neuropathy in cobalamin deficiency. Baillieres Clin Haematol, 1995; 8:479-497. 11.Schuitemaker GE. Van ‘open ruggetje’ naar ‘dementie’. Ortho 1995; 13:180-187. 12.VanTiggelenCJ.Vitamine B12 enhetzenuwstelsel. Orthomoleculair 1989; 7:178-180. 13.HirataF,AxelrodJ.Phospholipidmethylation and biological signal transmission. [Review]. Science 1980; 209:1082-1090. 14.Metz J. Cobalamin deficiency and the pathogenesis of nervous system disease. [Review]. Ann Rev Nutr, 1992; 12:59-79. 15.Weir DG, Molloy AM, Keating JN, et al. Correlation of the ratio of S-adenosyl-L-methionine to S-adenosyl-L-homocysteine in the brain and cerebrospinal fluid of the pig: implications for the determination of this methylation ratio in human brain. Clin Sci, 1992; 82:93-97.
19.VanTiggelen CJ. Microsomale levenre-nzymactiviteit. Orthomoleculair 1988; 6: 257-259. 20.LieberCS.Biochemical and molecular basisof alcohol-induced injury to liver and other tissues. New England J Med, 1986; 319:1639. 21.CarmelR,KarnazeDS,WeinerJM.Neurologic abnormalities in cobalamin deficiency are associated with higher cobalamin “analogue” values than are hematologic abnormalities. J Lab & Clin Med, 1988; 111:57-62. 22.Kanazawa S, Herbert V. Total corrinoid, cobalamin (vitamin B12), and cobalamin analogue levels may be normal in serum despite cobalamin in liver depletion in patients with alcoholism. Lab Invest 1985; 53:108-110. 23.Schaller H, Holler K. Thiamine absorption in the rat. Intl J Vitam & Nutr Res 1975; 45:31-38. 24Kwam-Fu Rex Sheu et al: Studies of trans-ketolase abnormality in Alzheimer disease. Arch Neurol, 1988; 45:841-846. 25.Enzi G. Folate status and cognitive impairment. [Review]. Aging 1994; 6:69-72. 26.Stokstad EL, Reisenauer A, Kusano G, Keating JN. Effect of high levels of dietary folic acid on folate metabolism in vitamin B12 deficiency. Arch Biochem & Biophys, 1988; 265:407-414. 27.Passeri M, Cucinotta D, Abate G, et al. Oral 5’-methyltetrahydrofolicacid in senileorganic mental disorders with depression: results of a double-blind multicenter study. Aging 1993; 5:63-71. 194 |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)