|

|
|
|
|
 Back to 1996 3rd Quarter Table of Contents
Back to 1996 3rd Quarter Table of Contents
Introduction In 1968 Linus Pauling introduced the word ‘Orthomolecular’ in his Science article,”Orthomolecular Psychiatry.” 1 With this report, now a classic, he announced to the world his entry into a new field of medicine, much to the discomfort of the medical profession and equally to the delight of the public at large. He had been familiar with the old vitamins-as-prevention paradigm, but within a brief period of time he had jumped into the vitamins-as-treatment paradigm, the modern paradigm which is sweeping into medicine so rapidly today. Adherents to the old paradigm accepted as articles of truth: (1) that vitamins were needed only to prevent vitamin deficiency diseases; (2) that only small quantities were required since they were catalysts; and (3) that they were contraindicated for every other condition not accepted as a vitamin deficiency disease. Within the past five years the medical profession has begun to distance itself from this paradigm. The modern paradigm is based on a different set of beliefs: (1) that vitamins are useful in a large number of conditions or diseases, not only to prevent vitamin deficiency diseases such as beri beri, pellagra or scurvy; (2) that they are needed in optimum, or orthomolecular amounts, which may be small or large.
1. 3A Quadra Street, Victoria, B.C. V8T 4E5 that niacin lowered serum cholesterol levels8 was the first major attack on the old paradigm, but only after our findings were confirmed by Parsons9,10 and his colleagues at the Mayo Clinic. We used doses up to three grams daily, about 300 times the recommended daily requirement, to lower cholesterol, which was not considered to be a vitamin deficiency disease. Linus Pauling’s book11, Vitamin C and The Common Cold, was the first report that engaged the attention of the whole world to the use of vitamins, in this case vitamin C, to the prevention and treatment of a disease not considered a vitamin deficiency disease. This was the first major frontal assault on the old paradigm and it elicited the expected reaction from its defenders. There was an enormous outpouring of rage from the medical establishment, as well as from dietitians and other adherents to the old paradigm. This rage colored most of the early attacks on Pauling. Thus, one author reported in an Australian journal that after Pauling had publicized the use of vitamin C there had been an enormous increase in the use of vitamin C, accompanied by a significant increase in the prevalence of kidney stones. The same journal rejected a critique I had written where I pointed out that using the author’s own statistics, it was clear that the increase in kidney stones was well developed long before Dr. Pauling made his original announcement and long before his book could have appeared in Australia, and that after the information became available there was no further significant change. They of course refused to publish my rebuttal. By 1968 fewer than 12 physicians and psychiatrists were using orthomolecular doses of vitamins. The first 500 mg tablets were made by a small company in Portland, Oregon, in 1960 as a favor to a California physician. He wanted to treat his twelve year old son who had been diagnosed as having untreatable schizophrenia. He had been advised to commit and forget him in a mental hospital. His son recovered in a few months and has been well since. He is a research psychiatrist. Dr. Humphry Osmond and I had organized the American Schizophrenia Association, later the Huxley Institute of Biosocial Research. By this time we were improving our patients’ nutrition as well as adding supplements of vitamins and minerals. We concluded that the term orthomolecular was just what we needed to create a division of medicine and psychiatry which would accurately draw attention to the kind of practices we were following. Dr. Pauling’s contribution was the largest single influence which kept orthomolecular medicine alive and growing. The medical conferences held over the past five years dealing with cancer and the use of nutrients would have been impossible without his brilliant and dedicated support to the development of the new paradigm. Dr. Linus Pauling and CancerIn 1979 Drs. Ewan Cameron and Linus Pauling published their book Cancer and Vitamin C,12 updated in 1993.13 This was the culmination of a number of reports published in the medical literature by both Cameron and Pauling. They found that as of August 10, 1976, all of the 1,000 control patients were dead, compared with 18 of the 100 treated with ascorbate who were still alive. The mean time of survival for the treated group was 4.2 times as great as it was for the control. They lived more than 300 days longer. Dr. J. Hoffer14 noted, in his recent analysis of this research, “the favorable effect of vitamin C in the Vale of Leven cancer patients, while not excellent, was far from negligible. Indeed it was comparable to the effect reported for IL-2 in later NCI-funded Phase II trials that attracted wide interest in the scientific medical community. Most important from the biologic perspective were the cases in which vitamin C induced catastrophic tumor hemorrhage and necrosis. Although IL-2 occasionally produces rapid remissions, it has never had an effect as dramatic as this.” The Cameron-Pauling studies were in effect an attack on the common cancer treatment paradigm and, therefore, were totally unacceptable. In 1977 a woman with obstructive jaundice was found at laparotomy to have an inoperable cancer of the head of the pancreas. She was given a bypass and advised she had only a few months to live. She had started to take ascorbic acid 10 g daily. When she told her physician, he advised her to see me. I increased her dose to 40 g and added other nutrients, since by that time I had been using multiple nutrients for psychiatric patients who were referred to me. Six months later her tumor was gone. She is still alive and well today. One case does not constitute proof but, like the white crow, it suggests that there is something there worth looking into. It shows that the rule that no cancers yield to nutrient therapy is wrong, in the same way that the rule all crows are black is no longer tenable. I then recalled two earlier patients, a retired professor15 who developed inoperable bronchiogenic cancer of the lung, for which he was given cobalt bomb radiation. He became psychotic. After two months with no improvement I started him on niacin, 3 g daily and ascorbic acid, 3 g daily. This was my standard treatment for this type of psychosis. He was mentally normal in four days. I continued him on the two vitamins until he died 30 months later. One year after he started, his lungs were clear. The cancer clinic saw a gradual recession of the lesion every three months. His lungs were clear after one year. About a year later I placed a 16 year old girl with Ewing’s sarcoma of the right arm on niacinamide 3 g daily and ascorbic acid, 3 g daily. She was booked for surgery to amputate her arm, but her surgeon was persuaded to wait for a month. She made a complete recovery and is still well 33 years later. I concluded that the main therapeutic factor was the vitamin B3 (niacin or niacinamide), as it is for schizophrenia.16 It does have anti-tumor properties.17,18 However, after studying Cameron and Pauling I was convinced that the main therapeutic nutrient was vitamin C, and that vitamin B3 had lesser anti-tumor properties. This case was significant, for it widened my practice of psychiatry by adding to it patients with cancer with significant depression and/or anxiety. The pancreatic cancer patient who had been cured publicized this fact widely to her friends, relatives and customers. Ironically, the only one who did not believe her was her younger brother, a psychiatrist, who knew vitamins could not help anyone. Gradually, physicians referred more patients to me until by 1988 I had seen 134. In 1985, after I had seen 41 patients, I realized that the patients given at least 12 grams of ascorbic acid daily had a better outlook. For patients seen between 1978 and 1983, out of 11 who did not follow the regimen none were alive and the mean survival was 4.8 months, while out of 26 who took the full dose of vitamin C, 18 were alive, for a mean survival of 16.2 months.19 A few years later at a Festschrift for Dr. Arthur Sackler, I discussed this data with Linus Pauling. He asked me if I intended to publish and I replied that I did not. I did not think I could persuade any medical journal to accept my paper. However he urged me to follow up each patient carefully and I agreed that I would. Two years later he asked me how I was getting along. I was embarrassed to admit I had not done what I had said I would do but, I added, I would do so immediately. I contacted every patient I had seen from 1978 to 1988, or their relatives or their physicians, or the cancer clinic. I sent this data to Dr. Pauling who analyzed it.20,21 In the first study22 134 patients seen between August 1977 and March 1988 were followed until December 31, 1989. We concluded that orthomolecular treatment given to female related cancers had improved life expectancy about 20 times compared to our non random controls and 12 times for other cancers. In our second paper23 a second cohort of 170 patients seen between April 1988 to December 31, 1989 was followed to December 31, 1992. These results were about the same as those we had earlier published. We concluded that while vitamin C alone led to about 10% excellent responders the addition of the other nutrients increased this to about 40%. I examined the first cohort of 134 further.24 In the first year after treatment, 75% of the control group of 33 died, compared to 25% from the treated group of 101. January 1, 1992, 41 patients were still alive from the treated group and one from the control. The average survival was 49 months for the treated group compared to 15 months for the control. The survival data suggested that the original Hoffer and Pauling estimates of survival were not far off the mark. As of December 31, 1993, 34 were still alive from the treated group and none from the controls. In order to obtain a comparison group we used the 33 patients from the original series of 134 who had not followed the program for at last two months. They represent the results of standard therapy which they had had or were still receiving. I have divided the group previously used as a control, into two control groups; (1) the group who did not live for two months after they first saw me - there were 14 and they lived on average 51 days; (2) the group who lived longer than 2 months and did not start on the vitamin program, of whom there were 19. They were alive on average 458 days or 15 months. The first group represents a terminal group who had failed to respond to standard treatment, or who had suffered a relapse after an initial response to previous treatment, and who may have been compromised by the treatment they had already received. It would have been desirable for patients who had decided for personal reasons never to accept any xenobiotic therapy to become a control group, but this was simply not possible in this study, nor would I recommend this to my patients for ethical reasons. As well, it is quite likely that some of the 101 patients in the treated group would also have died within that two month interval had they not been started on orthomolecular therapy, but this cannot be determined for these patients. Perhaps an equal number lived longer than two months as did those who did not make it for the two months after they first saw me. Taking all these factors into account, I think it is fair and reasonable to use the second control group as another valid comparison group, a concurrent group. This should also satisfy critics who maintain that every patient entered into the study must be retained in it, even if they did not follow the treatment protocol. Using this comparison group there were 101 patients who were able to follow the program, although some of them did not live very long after I first saw them. None were excluded from this group. The results of the treatment on the 101 can be compared with the results of the xenobiotic treatment on the 19. I now have seen over 750 patients in my series. With this enlarged sample it will be possible to examine these issues more thoroughly.25 I found that the difference between the vitamin treated patients and those who were not on the program was sustained. Survival of the two groups, the treated group of 101 and the pseudocontrol group of 19 treated only with xenobiotic therapy, is shown in Figure 1. The difference in outcome between these two groups remained large. In the first year, 75% of the group not on the orthomolecular program died, and at the end of five years 5% were alive. From the orthomolecular group 25% died by the end of the first year, and at the end of the 5th year 39% were alive. By January 1, 1992, 41 patients were still alive. The average duration of life from the time I first saw them until this date was 49 months, compared to 15 months for the group treated with xenobiotic therapy only. Pauling, as reported by J. Challem, Figure 1. Effect of Orthomolecular Treatment on Survival of Cancer Patients 120
|
| Q10 added | 13 | 1992 | 13 (100%) | 8(62%) |
|---|---|---|---|---|
| Not on Q10 | 55 | 1992 | 36 (65%) | 29(53%) |
| Q10 added | 37 | 92–93 | 32(86%) | Not available |
| Not on Q10 | 101 | 92–93 | 67(66%) |
entitled, Partial and Complete Remission of Breast Cancer in Patients in Relation to Dosage of Coenzyme Q10 in Nutritional Therapy, the authors reported an open trial of 18 months on 32 women with breast cancer of ‘high risk’. They were treated with 1.2 g of gamma-linolenic acid, 3.5 g of omega 3 essential fatty acids and 90 mg of Q10 daily. No patient died and all expressed a feeling of well being. They would have expected three to have died. In six there was a complete remission, less morphine was needed and distant metastases were not seen. In one patient they increased the Q10 to 300 mg daily after she had been on it for one year at 90 mg daily. Her tumor had stabilized at 1.5 to 2.0 cm. After three weeks on the higher dose it was gone. K.L. stated that in practicing oncology for 20 years and having treated countless cases of breast cancer he had never seen a spontaneous remission of this size and had never seen a comparable regression of any conventional anti-tumor therapy.
Based upon these observations I concluded that Coenzyme Q10 should be an integral component of all cancer therapy at the higher dose levels. If the cancer is entirely gone a lower maintenance dose probably would be adequate, perhaps 100 to 150 mg daily. It should be taken with the other vitamins and minerals.
Between November 1, 1993 and April 30, 1994 I started 43 patients on 300 mg of Q10 in addition to their usual nutrient program. During that same interval one patient died. For comparison I examined the same statistics for patients seen between November 1, 1992 and April 30, 1993. None of this group were receiving Q10. They were on the same program as were the group given Q10 one year later. Every patient seen during these intervals was included. From the earlier group of 32, 6 died within the same interval. Chi Sq for this distribution is 5.85, i.e. P < .02.
This is not a comparison of patients all seen after six months of treatment. The mean follow up was only three months, but both groups are treated equally. However it is rare in biological (especially human) studies, to achieve such a respectable probability of around two percent. It suggests that Coenzyme Q10 has in reality added something to the curative properties of the previous vitamin mineral regimen.
The one and two year survival for the smaller group of patients placed on Q10 is shown in Table 1.
After working with over 750 patients with cancer since 1978, I have no doubt that the orthomolecular program has improved the quality of their life. It has given them more energy, has eased depression and anxiety, has created a sense of well being, has eased pain and often has eliminated it entirely. So far not a single family has complained to me about the treatment and many have told me how grateful they were, for the program had made life so much more tolerable for them. A recent remarkable response will illustrate the effect of this program.
J.A. born in 1922 was seen January 6, 1994. She had a mastectomy in March 1990, right side. In March 1992 she developed low back pain which did not respond to chiropractic treatment or physiotherapy. In August 1992 she discovered a node in her neck. A bone scan showed two areas in the spine. She was given tamoxifen which made the pain intolerable and she would not take any more after five days against the wishes of her oncologist. After that she started on herbs and massage and was well in three months. September 1993 the pain recurred. Now she had metastases in her sternum and lower back. Pain in her chest was severe. She started on tamoxifen again and the pain again became intolerable. Two weeks later she started on ascorbic acid 15 g daily and on shark cartilage, but could only tolerate eight capsules of the cartilage. After starting vitamin C she slowly began to improve. She was able to leave her bed, but she still needed morphine every 12 hours.
I advised her to follow the orthomolecular program which included 15 g of ascorbic acid plus Coenzyme Q10, 300 mg. On February 1, 1994 she was free of pain and had discontinued the morphine. This she appreciated since the severe nausea generated by the morphine was gone. By February 23, 1994 the lumps had decreased to half their original size and she was able to move freely without pain. Both she and her husband were delighted.
Quality of life involves physical and emotional health. Physically a large number of symptoms will seriously interfere with the enjoyment of life. These include pain; restriction of movement; inability to function, for example to swallow; nausea and vomiting; loss of weight, appetite and the ability to meet energy requirements. I consider a person has a good quality of life when these factors are not present or are present to such a limited degree that they do not interfere with one’s lifestyle. Emotional health is equally if not more important.
The main changes in cancer patients are shock, depression, anxiety and the effect this mood has upon thinking and behavior. It is generated by the diagnosis, by the way it is given to them and by the knowledge that it is a major killing disease. One of the main problems is the fear shared by too many oncologists, surgeons and radiotherapists of the peculiar combination of words “false hope.” This is a basic contradiction of terms. There are various degrees of hope ranging from none to excessive. The term derives from the fear of the physicians that they will give a prognosis which is too optimistic and cannot be confirmed by follow up. They have gone to the other extreme and have been prone to give the patients zero hope.
Dr. William Osler, the famous Canadian-American physician, wrote about the importance of hope, and to illustrate it he told the following story about himself. He was asked to examine a man who had already been examined by two physicians who had advised the family that he would die that day. The family wanted another opinion. After his examination, Dr. Osler told the family that in his opinion the man would not die that day. But he did die that evening. The next morning the family approached Dr. Osler and thanked him profusely. He was, they said, the only physician who had given them some hope.
If there is anything at all to the placebo response, to the value of hope in the treatment of disease, then physicians must not remove this important variable. Even when it looks very grim indeed, the patient and family must be allowed some of the comforts of hope, but it must be realistic. It is essential not to exaggerate the hope. The patient should be advised that no matter how grim the situation is, there is some hope, and that the physician will help in any way possible. The best way to enhance hope is to be able to honestly report about other patients equally ill who have had their lives prolonged and the quality of life improved.
Levine30 describes the effect of hope on two cancer patients. A 55 year old woman was found to have an inoperable squamous cell carcinoma invading the mediastinal nodes. It was biopsied. The next morning the resident told her “Well, it’s cancer, and we couldn’t really resect it, so we just opened and closed.” She repeated, “opened and closed” several times. She died that night. At autopsy there was no specific cause of death. The resident had removed all hope.
The second patient had an aggressive T-cell immunoblastic sarcoma. He refused chemotherapy after being informed it likely would not help much. Dr. Levine, however, told him that there was a chance, albeit a slim one. He went into remission and was well for one year. Unfortunately the cancer clinics too often leave their patients bereft of hope. Recently I saw on follow up a man with lymphoma who is well after 3.5 years. He told me that when he was diagnosed the cancer clinic had told him there was nothing that could be done and that he had a very few months left. He and his wife left the clinic beaten and depressed. When he saw me recently he still was angry and resentful over the way they had treated him. I believe that after a patient leaves a doctors’ office he should feel better than when he entered. In most cases they leave their oncologists’ offices feeling much worse. They appear to encourage what I have called an obecalp reaction (placebo spelled backwards). If they are very depressed or anxious or suffer from any combination of these mood disorders I will treat them with the appropriate medication for this.
Recently Sapolsky31 in discussing the Measures of Life referred to the investigations of two psychologists, Amos N. Tversky of Stanford University and Daniel Kahneman of the University of California at Berkely. They investigated why people regard scenarios as unequal when in fact they are formally equivalent. He presented two scenarios: “You are a physician and you have a hundred sick people on your hands. If you perform treatment A, 20 people will die. If you opt for treatment B everyone has a 20% chance of dying.” and “You have a hundred sick people. If you perform treatment A, 80 people will live. If you opt for treatment B, everyone has an 80 % chance of living.” I was not surprised to learn that most people in the first scenario preferred treatment B and in the second one they preferred treatment A. Sapolsky wrote “The two scenarios are formally identical; they are merely framed differently. But it turns out that for the first scenario, which states things in terms of death, people will prefer option B, whereas for the second scenario, stated in terms of survivorship, people prefer option A. When thinking about life, people prefer certainty; when thinking about death, they prefer odds, because it is always conceivable the odds can be beaten.” My patients and I assume the vast majority of cancer patients prefer to bet on the odds they will survive and not on the certainty of death. The oncologists, surgeons, radiologists and physicians who treat these patients must take these observations to heart. These therapists can realistically convey to their patients that adding the orthomolecular component to the total treatment regimen will increase the probability they will survive longer and with a better quality of life. That is what patients with cancer want to know. They will be given, not false hope, but a realistic and accurate presentation of the facts. Patients will be able to follow their regimen more faithfully, and more comfortably.
The autonomic nervous system controls physiological responses to stress. Its chemical mediators on the sympathetic side are the catecholamines, dopamine, noradrenalin and adrenalin, particularly the last two. Dr. Cannon’s original description of the flight or fight mechanism is still valid. An emergency or a perceived emergency is a major stimulus to the autonomic nervous system which releases large amounts of adrenalin and noradrenalin. This prepares the body so it can respond best to the emergency. In animals an inadequate response will lead to either death (the victim), or to no meal (the predator). A rabbit which responds optimally may escape. A coyote which responds optimally may have a meal. Adrenalin alerts the body, increases heart rate and blood pressure, increases the rate of breathing and diverts blood from viscera to the muscles where it is most needed. It increases sweating to cool the body. It decreases the sensation of pain. This physiological response has been developed over billions of years and is still fully functional even though civilized mankind very seldom has the same need to respond to emergencies the same as do animals in the wild.
Adrenalin is very toxic because it elevates the blood pressure. The body must remove it as quickly as possible. To do so it has developed two main pathways for converting it to other substances.32,33,34 One pathway leads to adrenochrome which does not elevate blood pressure. The other pathway leads to non indolic derivatives. The second pathway is controlled by several enzymes called amine oxidases. Thus a highly reactive compound which elevates pressure is replaced by other compounds that do not have this property.
But adrenochrome (and the other chrome indoles from noradrenalin and from dopamine) have other properties. Adrenochrome is a mitotic poison, i.e. it decreases the rate of cell division. In heart muscle and in leukocytes about 80% of the adrenalin is converted into adrenochrome. And adrenochrome is toxic in other ways. It is an hallucinogen. This is fully described in our book “The Hallucinogens35(1967). There we discussed its biochemical, physiological, and psychological properties. It is a highly reactive compound with a short half-life in the body where it is quickly converted into adrenolutin, 3,5,6 tri hydroxy N-methyl indole, which is also hallucinogenic and to 5,6 dihydroxy N-methyl indole which is not. On the contrary this compound, also called leuko adrenochrome (white adrenochrome), has good anti-anxiety properties. These substances circulate in the body. The hallucinogenic properties of adrenochrome and adrenolutin led to our adrenochrome hypothesis of schizophrenia36–45 i.e. that this disease came about due to the increased formation of these oxidation products of adrenalin. For the rest of this discussion I will consider its anti mitotic properties and its hallucinogenic properties.
In our 1967 discussion35 we wrote “Adrenochrome markedly inhibits mitotic rate of cells, probably by interfering in the glycolytic cycles. Bullough found that when mice were stressed by overcrowding, the adrenal medulla increased in size 80%. At the same time the epidermal mitotic rate fell 60%. In vitro adrenaline had no anti mitotic effect on epidermis but when it was injected it did. In contrast adreno-chrome was anti mitotic both in vitro and in vivo. Bullough suggested that during stress the increased quantity of adrenaline was converted into adrenochrome which produced the antimitosis.”
These two properties, antimitosis and hallucinogenic, suggest that adrenochrome is involved in two conditions (a) the control of mitosis in the body; (b) schizophrenia. Elsewhere I46 have suggested that schizophrenia is a defense mechanism against stress which has gone too far. It is highly likely that since adrenochrome is present in the body that it would be used to control excess mitosis and that it is involved in the prevention of cancer. This is the hypothesis I will elaborate, i.e that too little adrenochrome will increase incidence of cancer and decrease the incidence of schizophrenia, while too much will decrease the incidence of cancer and increase the incidence of schizophrenia.
Small amounts of adrenalin are produced all the time, even during sleep, but during the day and when exposed to stress the amount is increased. The continual, even if fluctuating level of adrenalin will ensure a constant production of adreno-chrome and its conversion to adrenolutin and other indoles. I suggest that this is one of the mechanisms the body uses to deal with excess mitotis. The leukocytes probably destroy abnormal cells by releasing adrenochrome which has the properties of a free radical and will destroy the cell. It is recognized that pro oxidants are needed to destroy cancer cells. Adrenochrome is probably the best and safest natural pro oxidant in the body. This hypothesis suggests a number of testable sub hypotheses.
A) A deficiency in the production of adrenochrome will increase the incidence of cancer and decrease the incidence of schizophrenia. This can arise from (1) inadequate production of adrenalin (2) a deficiency of enzymes which convert adrenalin to adrenochrome (3) a deficiency of oxygen and (4) a deficiency of auto oxidizing systems such as copper or iron.
A deficiency of adrenalin can arise from a deficiency of tyrosine but this is highly unlikely. It can also arise from extirpation of the adrenal glands, one of the major sources of adrenalin. It could arise from a lack of stimulation of the sympathetic nervous system. Factors such as staying in bed all day would decrease the need for adrenalin to help control blood pressure. An absence of challenges to the body both psychological and physical could also produce a deficiency of adrenalin. It could also come about by the use of anti anxiety drugs and tranquilizers which effectively isolate the individual from stress. Infections are stressful and increase the activity of the immune system. The use of tranquilizers since 1950 has effectively removed this spur to the immune system for many people and may be another factor in decreasing adrenalin and therefore adrenochrome production. Helen Coley Nauts47 made the very sensible suggestion that the loss of repeated episodes of infection by bacteria since the introduction of antibiotics may be a major factor in the rising prevalence of cancer in the highly industrialized world. According to this hypothesis repeated infections acted as a spur to continually reinvigorate the immune system. According to the adreno-chrome hypothesis it would act as a spur to increase the production of adrenochrome.
B) Excessive formation of adreno-chrome will decrease the prevalence of cancer and will increase the prevalence of schizophrenia. This can arise from the following factors (1) An overproduction of adrenalin for prolonged periods of time due to excessive stress of various types, (2) an increase in the production of adreno-chrome due to an increase in the conditions which favor this reaction such as more of the oxidizing enzymes, too little activity of the other enzymes which convert adrenalin to other non indolic substance, an increase in oxygen tension, an increase in oxidizing metals such as copper or iron and finally too much inhibition of the reaction by any factor which would normally take adrenalin down the non adrenochrome pathway.
If cancer did develop in a schizophrenic person it would probably be less invasive and easier to treat with a better outcome. Patients with cancer would be less likely to become schizophrenic and patients with schizophrenia would be less likely to get cancer.
Both of these propositions are true.
Since 1977 I have examined and treated over 750 patients with cancer covering almost the entire spectrum of types of cancers and organs involved. Only five were schizophrenic. Three had cancer of the breast, one had a lymphoma and one cancer of the thyroid. In every case the response to treatment was excellent. They are all alive, averaging six years. The usual stated life time incidence of schizophrenia is said to be 1%. I think it is closer to 2 %. Therefore I would expect that out of this series I would have seen more than these five. Kanofsky48 (1994) concluded that schizophrenic patients have a lower incidence of lung cancer compared to the general population even though they are much heavier smokers. He also found that smoking did not lower their ascorbic acid blood levels as much as it does in other people. This he thought lowered their risk on exposure to smoking but according to this adrenochrome hypothesis it might equally have arisen from the increased concentration of adrenochrome. Kanofsky pointed out on the basis of a literature search that in general schizophrenics have a higher death rate than do the general public. Some studies have shown they have a greater rate for non lung cancer and a lesser or greater rate for all other cancers. The earlier literature had concluded that cancer was rare in schizophrenics who were catatonic and hebephrenic, terms no longer in general use. On the contrary, the death rate from cancer in paranoid schizophrenics was higher than it was in the general population. The only clear finding is the decrease in lung cancer. Perhaps if they were non smokers their rate of lung cancer would be even lower.
I have seen over 4,000 schizophrenic patients since 1952. Currently I have at least 500 chronic patients under my care. The total incidence of cancer is very low. From my current list only five have cancer, the same five that I referred to in the cancer series. A few characteristics of this group is shown in Table 2.
If adrenochrome is synthesized in greater amounts in schizophrenia, during remission (spontaneous or due to treatment) there may not be enough adreno-chrome to prevent the cancer from appearing but enough to greatly enhance their prognosis. They have all recovered from their cancer. The lymphoma patient is still free of cancer but he is not well mentally.
From the much larger series I treated I cannot recall any cases of cancer. I would expect a much higher incidence of cancer in the schizophrenic group unless there was this incompatibility between the two conditions.
There is other evidence as well. Professor Rudy Falk,49 University of Toronto Medical School, formerly Chief of Oncology at St. Michael’s Hospital, Toronto, estimated that he had seen over 25,000 patients during his long career and Dr. J. Holt,50 an oncologist in Australia had seen nearly 18,000 patients over his 41 years of practice. They cannot recall a single patient who was also schizophrenic. Dr. Holt had been puzzled by this incompatibility for many years. Out of nearly 48,000 cases only five are known to have had schizophrenia. Dr. Holt’s group also had treated
Table 2. A Few Characteristics of the Group With Both Cancer and Schizophrenia
| Number | Sex |
| 1 | F |
| 2 | F |
| 3 | F |
| 4 | F |
| 5 | M |
Type Schiz first Alive, years
| Breast | Yes | 4 |
| Thyroid | Yes | 4 |
| Breast | Yes | 6 |
| Breast | Yes | 2 |
| Lymphoma | No | 12 |
about 700 patients with Ankylosing Spondylitis and he estimated about six had been schizophrenic with another 12 disturbed psychiatrically. Apparently this physical condition did not protect against schizophrenia.
It occurred to me that this protective effect might also be found in the most closely related relatives of these patients i.e. parent, siblings and children. These relatives do have some evolutionary advantage.51 Over the past year I have asked each cancer and each schizophrenic patient I have seen about the presence of either condition in their first order relatives. The results of this clinical survey are shown in Table 3.
Chi Sq. for the distribution for the last two columns is 18 i.e. P<.001. For the distribution of schizophrenic patients only between the two groups it is 11.1 and for cancer cases only it is 22.
About 12% of the cancer relatives developed cancer. From the schizophrenic relatives only six percent did. From the cancer relatives only two (0.4%) had schizophrenia. The incidence among the general population is between one and two percent which from this group should yield between five and ten patients. And from the schizophrenic relatives 12 had cancer. This data supports the hypothesis i.e. that patients liable to get cancer are much less apt to get schizophrenia and that patients who have or have had schizophrenia are much less apt to have had cancer. Patients with a predisposition to cancer do not make enough adrenochrome to become psychotic, while other people who only make enough adrenochrome now and then will get schizophrenia and will be protected to a degree from getting cancer. And schizophrenic patients who do get cancer will have a much better outlook with treatment.
This inverse association between these two killing diseases, cancer which destroys life and schizophrenia which destroys normal life, leads to the prediction that if a patient has cancer and then develops schizophrenia the cancer will be destroyed by the adrenochrome.
Perhaps my first cancer case in 1960 who was psychotic for at least two months represents one of these cases. Perhaps his recovery was due to the combination of his psychosis which cleared very rapidly on niacin and ascorbic acid, the vitamins and the cobalt bomb radiation.
Brown and Foster52 examined the geographical relationship between the prevalence of schizophrenia and selenium deficiency in the soil. Their careful detailed examination of nine surveys led to the conclusion that there is a connection between selenium deficiency and the prevalence of schizophrenia and to the suggestion that selenium supplementation might be valuable in preventing and treating schizophrenic patients. There is also a similar relationship between the prevalence of esophageal cancer and selenium deficiency. This appears to suggest that both schizophrenia and cancer ought to be positively related and they are not. It is possible that a deficiency of selenium increases the probability of developing both diseases but that it plays a much greater role in preventing cancer. Thus both are increased in the absence of
Table 3. The Presence of Cancer and Schizophrenia in First Order Relatives of Patients With Cancer or Schizophrenia
Schizophrenia 79 382 12 22 Cancer 80 529 2 61
enough selenium but at the same time the association between the two diseases is negative.
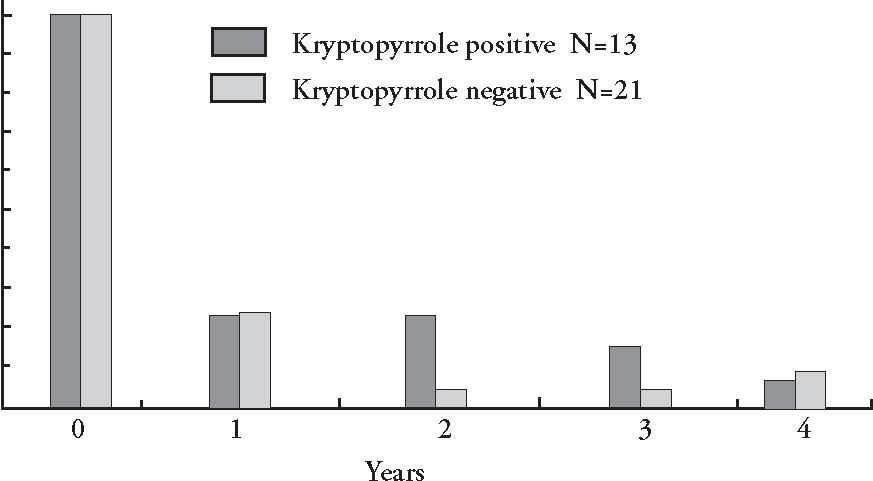
Kryptopyrrole(KP) is found in the urine of the majority of schizophrenic patients and in very few normal people. (See Eva Edelman53 for a comprehensive review of kryptopyrrole). It is highly correlated with schizophrenia and its presence established the diagnosis, pyrolleuria. It is also present in some patients with cancer, especially if they have cancer of the lung. Seven out of eight patients with lung cancer were positive for KP while four out of four tested after treatment were negative. Two of seven ovarian and uterine cancer patients were positive. From both groups 80% had pyrolleuria. But from all other cancers 24 out of 79 or 30% were positive. In my review54 of the psychophysiology of cancer I summarized the cancer literature which showed that lung and ovarian cancers had the highest incidence of psychotic change, usually a form of dementia. This group also had the highest incidence of KP in their urine.
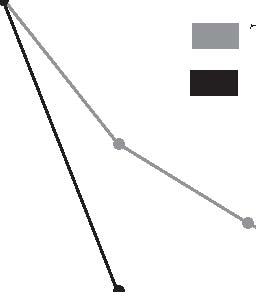
This puzzled me for many years. In thinking about these results it occurred to me that perhaps the presence of this factor might have an effect on survival. I examined the urine of 34 cancer patients for KP. Only one had been given any vitamin therapy. Thirteen excreted KP and they survived 647 days after their urine was tested. Four lived at least three years. The mean survival of the 21 without the factor was 297 days. Three lived at least three years. This is shown in Figure 3.
If the adrenochrome hypothesis is valid there will be a correlation between schizophrenia and adrenochrome formation and also between this disease and the presence of KP in the urine. Thus the presence of KP would be a marker for increased adreno-chrome formation. Is this why they survived longer? Dr. O. O’Reilly, a research colleague also examined urines for KP and he found that cancer patients with KP lived 40 days longer on average than patients who were negative. This was a ten percent increase in longevity in cancer patients none of whom were treated with vitamin supplements.
To control cancer one needs two sets of reactions (1) pro-oxidants e.g. adreno-chrome, which are used by the body to destroy the tumor cells. Leukocytes kill by
Figure 3. Kryptopyrrole and Cancer Survival
100 90 80 70 60 50 40 30 20 10
0
discharging free radicals into the bacteria or cell they are attacking. Adrenochrome is a natural superb free radical. (2) Anti-oxidants to neutralize the free radicals as soon as their work is done to prevent injury to other cells and tissues. The adrenalin-adrenochrome system provides a very good system for controlling mitosis. The adrenalin is maintained by repeated exposure to stress. The adrenalin is converted to adrenochrome and is used by the body as needed and the excess is neutralized by conversion into other indoles which are not as toxic. This is done by the natural anti-oxidants such as ascorbic acid, vitamin E, the carotenes and other anti oxidants found in food.
Increase the production of adrenalin.
several physicians with some success.
(c) Hyperthermia. This should also increase the secretion of adrenalin and therefore of adrenochrome.
(b) Using adrenochrome derivatives.55–57
Why are vitamin B3 and these antioxidants therapeutic for a large variety of conditions? Both vitamin C and vitamin B3 have an enormous range of therapeutic activities.60–66 This suggests that except for the two diseases cancer and schizophrenia, which have a direct relationship to adreno-chrome, these vitamins have a general systemic effect which reduces the body’s pathological reaction to stress and thus allows the natural repair processes of the body to operate at a more efficient level. Since every disease results from or creates stress on the body because of the impact of increased production of adrenalin and adrenochrome these anti stress vitamins should have a general therapeutic effect on every disease. Every disease, or every stress related activity will benefit from the addition of optimum amounts of the B-vitamins especially B3 and the anti-oxidant nutrients including vitamin C, vitamin E, the carotenes, Coenzyme Q10 and the anti-oxidant trace element selenium. There is already ample evidence in addition to the evidence presented here that life is extended and its quality enhanced by this program. Niacin prolongs life,67 vitamin E should do so as it decreases the frequency of coronary disease,68,69 and vitamin C prolongs the life of cancer patients. They each work when used alone but there is a growing consensus that the combination of these anti-oxidants has a synergistic effect.70 Prasad,71 using cell cultures, found that using individual vitamins might be effective, ineffective or even counter productive depending upon the vitamin, dose and type of tumor. In contrast the mixture of four vitamins (vitamin C, alpha tocopherol succinate, beta carotene and retinoic acid) consistently reduced growth of both cell lines studied and enhanced the growth inhibitory effects of chemotherapeutic agents on these cells. Unprocessed food does not contain only one vitamin. It contains them all even if in very small amounts. It is not surprising that they work better in combination with each other for that is what nature has been doing since life originated.
Parkinson’s disease is another example of a condition which is related to excessive oxidation72–76 (auto-oxidation), yielding too many free radicals. Jenner76 writes “There has been reluctance by scientists, grant-giving bodies, and the pharmaceutical industry to accept that free-radical mechanisms are an important component of neurodegenerative disease. A decade ago the concept was thought facile but at least now some acceptance has been gained. Nobody is claiming that free radicals explain every unique feature of neurodegenerative disease. Rather, we are proposing that they are a common feature of the process of cell death in most, if not all, such illnesses. If so, the therapeutic rewards may be great. It may become possible to stop or slow the progression of common disorders, such as Alzheimer’s or Parkinson’s disease, with a single therapeutic approach.”
I have evidence that the combination of niacin (and perhaps niacinamide as well) and anti-oxidants will be therapeutic for Parkinson’s disease. Over the past thirty years I have treated patients with Parkin-son’s disease with niacin, 500 to1000 mg tid. It has been very effective in removing psychiatric symptoms but has been of no value in treating the neurological component. This disease is considered to be a dopamine deficiency disease and is treated with large doses of l-dopa, in one form or another. But large doses produce schizophrenic-like symptoms, the higher the dose the greater the incidence.77,78 This is not surprising since dopachrome must have properties similar to adrenochrome, i.e. is an hallucinogen. More likely Parkinson’s disease is a combination of too little dopamine and too much dopachrome i.e. there is excessive conversion of dopamine into dopachrome. Dopachrome is neuro-toxic and by increasing destruction of neurons will accelerate the development of the disease while at the same time masking some of the symptoms. Adrenalin is oxidized to oxidized adrenalin losing one electron. In the presence of the NAD<——>NADH system the oxidized adrenalin is reduced back to adrenalin and the cycle continues. When there is too little NAD or NADH or both another electron is lost and adrenochrome is formed. This last reaction is irreversible. Vitamin B3, therefore, can decrease the production of adrenochrome. This has not been tested experimentally but in a recent series of reports, Professor J. G. D. Birkmayer and his associates at the Birkmayer Institute for Parkinson Therapy, in Vienna, Austria, studied a stable form of NADH. They found that their stable preparation using 5 mg doses was therapeutic for Parkinson’s disease, for Alzheimer’s, and for depression.79–82They wrote, “When we first used NADH with regard to its clinical efficacy the effect was not convincing. This was most likely due to the rapid dissolution (approximately 10-15 minutes) of the capsule leading to a release of NADH into the acid conditions of the stomach. Since NADH is rapidly oxidized below pH 7.6 the conditions in the stomach will inactivate NADH by converting it to NAD. The investigations of this report were therefore performed with NADH capsules coated with an acid stable film and a release time of two to three hours. With this galenic formulation of NADH an improvement in disability could be achieved which was comparable to that of intravenously applied NADH.”
The lipid soluble vitamin E has some therapeutic value in treating Parkinson’s disease. Coenzyme Q10 is coming into prominent use as a powerful anti-oxidant. Schapira et al 83 reported that NADH-ubiquinone (Q10) reductase (Complex 1) and NADH cytochrome c reductase activities were reduced in Parkinson’s disease in the substantia nigra. It occurred to me that providing both increased amounts of niacin, the precursor of NAD and NADH, and large amounts of coenzyme Q10, would be of value in treating cases of Parkinson’s disease. I have given this combination to one patient with classical Parkinson’s disease. The first one, age 84, had been on the orthomolecular regimen for at least 25 years and he was mentally normal. His program included niacin 1 gram tid and the usual anti-oxidants such as ascorbic acid, vitamin E, selenium. A couple of years ago Parkinson’s disease was diagnosed. It was evident in his gait, leg muscle weakness and tremor. Last year his neurologist started him on SinemetTM which may have helped slightly but he continued to deteriorate. Late last summer I advised him to add coenzyme Q10, 600 mg daily to his program. Within two weeks he was much better. When I saw him early in July this year he had regained the use of his limbs, had very little tremor and was able once more to play golf as had been his habit before. He is on Q10, 300 mg daily. His neurologist was very surprised at the marked improvement.
Another patient had difficulty walking for many years. Her walk closely resembled the walk of a patient with Parkinson’s disease and the diagnosis had been considered by her physician. I tried to help her for several years with no relief. But after she was started on Q10 300 mg daily, within one month there was a marked improvement in her walk and also in her mood.
With a combination of vitamin B3 plus anti-oxidants, especially Q10, it may be possible to prevent and to treat Parkinson’s disease. The treatment would have to be started as early as possible before too many neurons have been destroyed by the adreno-chrome or dopachrome. The niacin will protect against the psychological side effects of the l-dopa treatment and the anti-oxidants will protect against the neuromuscular effects of the disease. One could then use l-dopa without the patient having to suffer its toxic consequences and their lives would be prolonged.
1) The survival trends which appeared in the first Hoffer and Pauling paper, and reappeared in our second one and in my third presentation, are reconfirmed in this report. From 101 patients on the program, a core of 33 patients remain alive as of July 1, 1996. Of these 33, 24 have lived 10 years, and seven more will probably live 10 years. The ten year survival will probably be 30% out of the original group. Over half of the seven 1992 deaths were due to non-cancer physical causes. It is likely further deaths will come increasingly from other causes.
2) This conclusion applies only to patients who have received a combination of all the standard modalities of treatment and orthomolecular treatment.
3) The estimated survivals from the first Hoffer and Pauling report are confirmed by the actual and expected future survivals of these groups.
4) Better results were found with patients who were placed on the combination soon after they were diagnosed and standard treatment was started. Adding coenzyme Q10 improved the results by about ten percent.
5) Arbitrarily I have concluded that there must be a minimum two month period on the nutritional program before it can begin to demonstrate its ability to prolong life. More study will be required to determine what is the minimum period.
6) The program is palatable. The only patients who could not follow it were those who were getting chemotherapy and suffered severe nausea and vomiting, or patients who could not swallow because of lesions in their throats.
7)Orthomolecular treatment improves the quality of life. It also decreases the side effects of radiation and chemotherapy.
8)Orthomolecular therapy provides a step forward in the battle against cancer which must be fully explored. There can be no logical reason today why most of the research funds should go toward the examination of ever more chemotherapy of the standard kind and more ways of giving radiation. There must be a major expansion in the use of orthomolecular therapy, to sort out the variables and to determine how to improve the therapeutic outcome of treatment.
9)Enterprising medical schools should immediately consider establishing chairs in Orthomolecular Oncology. I recommend that there should be at least one Linus Pauling Chair of Orthomolecular Oncology.
10) I have proposed a hypothesis to account for the apparent incompatibility between schizophrenia and cancer, using the adrenochrome hypothesis as the basis.
I: Treatment of Schizophrenia with Nicotinic Acid and Nicotinamide. J Clin Exper Psychopathol, 1957; 18:131-158.
Proc. Staff. Meet. Mayo Clin 1956; 31: 377-90.
10.Parsons WB: Clinical alternatives. coronary heart disease. In ed. GV Mann: The Dietary Sense and Nonsense.An Evaluation by Scientists. Great Britain, Janus Publishing Co. 1993.
11.Pauling L: Vitamin C and The Common Cold, San Francisco, WH Freeman, 1971.
12.Cameron E & Pauling L: Cancer and Vitamin C. Palo Alto, CA, Linus Pauling Institute of Science and Medicine, 1979.
13.Cameron E & Pauling L: Cancer and Vitamin C. Updated and Expanded. Philadelphia, Camino Books, 1993.
14.Hoffer J: Nutrients as biologic response modifiers. In ed. P Quillin & RM: Adjuvant Nutrition in Cancer Treatment. Williams. 1992 Symposium Proceedings, Cancer Treatment Research Foundation and American College of Nutrition, Cancer Treatment Research Foundation, 3455 Salt Creek Lane Suite 200, Arlington Heights, IL 60005-1090, 1993.
15.Hoffer A: Treatment of organic psychosis with nicotinic acid (A Single Case). Dis Nerv Syst, 1965; 26: 358-360.
16.Hoffer A, Osmond H, Callbeck MJ & Kahan
I: Treatment of schizophrenia with nicotinic acid and nicotinamide. J Clin Experim Psychopathol, 1957; 18:131-158.
17.Jacobson EL: Niacin deficiency and cancer in women. J American College of Nutrition 1992;
11: 597-637.
18.Jacobson EL & Jacobson MK: A biomarker for the assessment of niacin nutriture as a potential preventative factor in carcinogenesis. J Intern Med , 1993; 233: 59-62.
19.Hoffer A: Orthomolecular Medicine for Physicians. New Canaan, CT, Keats Publ. 1989.
20.Pauling L: Biostatistical analysis of mortality data for cohorts of cancer patients. Proc Nat Acad Sci USA, 1989; 86:3466-3488. 21.Pauling L & Herman Z: Criteria for the validity of clinical trials of treatments of cohorts of cancer patients based on the Hardin Jones principle. Proc Nat Acad Sci USA, 1989; 86: 6835-6837.
22.Hoffer A & Pauling L: Hardin-jones bio-statistical analysis of mortality data for cohorts of cancer patients with a large fraction surviving at the termination of the study and a comparison of survival times of cancer patients receiving large regular oral doses of vitamin C and other nutrients with similar patients not receiving those doses. J Orthomolecular Medicine, 1990; 5:143-154.
23.Hoffer A & Pauling L: Hardin-jones biostatistical analysis of mortality data for a second set of cohorts of cancer patients with a large fraction surviving at the termination of the study and a comparison of survival times of cancer patients receiving large regular oral doses of vitamin C and other nutrients with similar patients not receiving these doses. J Orthomolecular Medicine, 1993; 8: 1547-1567.
24.Hoffer A: Orthomolecular Oncology. In ed. P Quillin & RMWilliams, Adjuvant Nutrition in Cancer Treatment. Cancer Treatment Research Foundation, 3455 Salt Creek Lane Suite 200, Arlington Heights, IL 60005-1090: 1994.
25.Hoffer A (With Major Contributions by Linus Pauling), Quarry Press, in press (due 1997).
26.Pauling L: Quoted in “The Nutrition Reporter” Challem J, 1992; 3: 8.
27.Hoffer A: Orthomolecular oncology and survival. Adjuvant Nutrition in Cancer Treatment Symposium. San Diego, CA, March 17-19, 1994.
28.Bliznakov EG & Hunt GL: The Miracle Nutrient Coenzyme Q10. Toronto. Bantam Books, 1987.
29.Folkers K, Brown R, Judy WV & Morita M: Survival of cancer patients on therapy with Coenzyme Q10. Biochem Biophys Res Comm, 1993; 192: 241-245.
30.Levine AM: The importance of hope. West J Med, 1989; 150: 609.
31.Sapolsky RM: On human nature. The Sciences 1994; 34:10-14.
32.Matthews SB, Henderson AH & Campbell AK: The adrenochrome pathway: The major route for adrenalin catabolism by polymor-phonuclear leucocytes. J Mol Cell Cardiol 1985; 17: 339-348.
33.Bindoli A, Rigobello MP & Deeble DJ: Biochemical and toxicological properties of the oxidation products of catecholamines. Free Radical Biology & Medicine 1992;13: 391- 405.
34.Dhalla KS, Ganguly PK, Rupp H, Beamish RE & Dhalla NS: Measurement of adrenolutin as an oxidation product of catecholamines in plasma. Molecular and Cellular Biochemistry 1989; 87: 85-92.
35.Hoffer A & Osmond H: The Hallucinogens. New York, Academic Press, 1967.
36.Hoffer A, Osmond H & Smythies J: Schizophrenia: A New Approach. II. Results of a Year’s Research. J Ment Science 1954;100: 29-45.
37.Hoffer A: Adrenochrome and adrenolutin and their relationship to mental disease. In eds. Garattini S & Ghetti V: Psychotropic Drugs. London, Elsevier Press, 1957; 10-20.
38.Hoffer A: The effect of adrenochrome and adrenolutin on the behavior of animals and the psychology of man. Int Rev Neurobiol
ogy 1962; 4: 307-371.
39.Hoffer A: The adrenochrome hypothesis of schizophrenia revisited. J Orthomolecular Psychiatry 1981;10: 98-118.
40.Hoffer A: Oxidation-reduction in the brain. J Orthomolecular Psychiatry, 1983; 12: 292-301.
41.Hoffer A & Osmond H: The adrenochrome hypothesis and psychiatry. J Orthomolecular Medicine, 1990; 5: 32-45.
42.Smythies J: On the function of neuromelanin. Proc Roy Soc (London) B2, 1996; 63: 491-496.
43.Smythies J: Hallucinogenic drugs. Encyclopedia of Neuroscience. In press, 1996.
44.Smythies J: The role of ascorbate in brain: therapeutic implications. J Roy Soc of Med 1996; 89: 241.
45.Smythies J: Disturbances of one-carbon metabolism in neuropsychiatric disorders: a review. Submitted to Biological Psychiatry, 1996.
46.Hoffer A: Schizophrenia: An Evolutionary defence against severe stress. Townsend Letter for Doctors and Patients #151/152 Feb/Mar 1996.
47.Nauts HC: Bacterial products in the treatment of cancer: past, present and future. In eds. Jeljaszewics J, Pulverer G, Rostowski W: Bacteria and Cancer, New York. Academic Press 1982.
48.Kanofsky JD, Norkus EP, Geller B, Lowinger R, Kanofsky PB & Kennedy GK: Schizophrenia, lung cancer and vitamin C. American Psychiatric Association, Poster Session, Philadelphia, May 1994.
49.Falk R: Personal communication, 1995.
50.Holt JAG: Letter, September 21, 1993, Microwave Therapy Center, 311 Outram St.,
W. Perth, Australia, 6005.
51.Huxley J, Mayr E, Osmond H & Hoffer A: Schizophrenia as agenetic morphism. Nature, 1964; 204: 220-221.
52.Brown JS & Foster HD: Schizophrenia: an update of the selenium deficiency hypothesis. J Orthomolecular Medicine, In press, 1996.
53.Edelman E: Natural Healing for Schizophrenia. A Compendium of Nutritional Methods. Eugene, OR, Borage Books, 1996.
54.Hoffer A: The psychophysiology of cancer. J Asthma Res, 1970; 8: 61-76.
55.Nakatsugawa S & Sugahara T: Differential action on cancer and normal tissue by adrenochrome monaminoguanidine methane-sulfonate and cytochrome C combined with radiotherapy. Int J of Radiation Oncology, Biology, Physics 29:635-638, 1994.
56.Sugamoto K, Kimura H, Kawashima H, Itojima T, Aoyama T & Sugahara T: Radioprotective effects of adrenochrome monoamino-guanidine methanesulfonate (AMM) on irradiated C57B1 mice and the survival of GM-CFC, a hemotopoietic progenitor cell. J Radiat Res, 29:211-219, 1988.
57.Yamashita H, Okura J & Izumi K: Protective effect of adrenochrome monoguanylhydrazone methanesulfonate (S-Adchon) on the hematopoietic organ as revealed in irradiated cancer patients. J Radiat Res 12:41-50, 1971.
58.Kim JH, Kim SH, He S, Dragovic J, Brown
S: Use of vitamins as adjunct to conventional cancer therapy. Second Denver Conference on Nutrition and Cancer, Denver, CO, Sept 7-11, 1994. In Nutrients in Cancer Prevention and Treatment. Eds. Prasad KN, Santamaria L & Williams RM, Humana Press, New Jersey, 363-372, 1995.
59.Agnew N & Hoffer A: Nicotinic acid modified lysergic acid diethylamide psychosis. J Ment Science, 101:12-27, 1955.
60.Stone I: The Healing Factor: Vitamin C against Disease. Grosset and Dunlap, New York, 1972.
61.Pauling L: How To Live Longer and Feel Better. WH Freeman and Company, New York, NY, 1986.
62.Hoffer A: Vitamin B3 (Niacin). Keats Pub, New Canaan, CT, 1984.
63.McCracken RD: Niacin and Human Health Disorders. Hygea Publishing Co., 635 Peterson St., Fort Collins, CO, 80524.
64.Hoffer A & Walker M: Smart Nutrients - A Guide to Nutrients That Can Prevent and Reverse Senility. Avery Publishing Group, Garden City Park, NY, 1994.
65.Hoffer A: Hoffer’s Law of Natural Nutrition. Quarry Press, Kingston, ON, 1996. 66.Hoffer A & Walker M: Putting It All Together
The New Orthomolecular Nutrition. Keats Publishing Inc, 27 Pine Street, Box 876, New Canaan, CT 06840-0876, 1994.
67.Canner PL, Berge KG, Wenger NK, Stamler J, Friedman L, Prineas RJ, Friedewald W: Fifteen year mortality in coronary drug project patients: long-term benefit with niacin. J Amer Coll of Cardiology, 8:1245-1255, 1986.
68.Rimm EB, Stampfer MJ, Ascherio A, Giovannucci E, Colditz GA & Willett WC: Vitamin E consumption and the risk of coronary heart disease in men. New England J Med 1993; 328: 1450-1456. In this paper there is no reference to the work done by the Shute Brothers in Ontario about 50 years ago. Their work had already established the enormous value of vitamin E in the treatment of coronary disease and other diseases.
69.Stampfer MJ, Hennekens CH, Manson J, Colditz GA, Rosner B & Willett WC: Vitamin E consumption and the risk of coronary disease in women. New England J Med 1993;
328: 1444-1449.
70.Prasad, KN Chairperson. Second Denver Conference on Nutrition and Cancer. Sept 7 - 11, 1994, Denver, Colorado. In eds. Prasad N, Santamaria L & Williams RM: Nutrients in Cancer Prevention and Treatment. New Jersey, Humana Press, 363-372, 1995.
71.Prasad KN: Cellular basis of using multiple antioxidant vitamins in cancer prevention and treatment. Nutrition in Cancer Treatment Symposium, Tampa, Florida, 1995.
72.Fornstedt B: Role of catechol autooxidation in the degeneration of dopamine neurons. Acta Neurol Scand,Suppl. 1990; 129: 12-14.
73.Mann DMA & Yates PO: Possible role of neuromelanin in the pathogenesis of Parkinson’s disease. Mech Age Dev, 1983; 21: 193-203.
74.Olanow CW: Oxidation reactions in Parkinson’s disease. Neurology 40 (Suppl 3) 1990: 32-38.
75.Fahn S & Cohen G: The oxidant stress hypothesis in Parkinson’s disease: Evidence supporting it. Annals Neurology,1992; 32:804-812.
76.Jenner P: Oxidative damage in neuro-degenerative disease. The Lancet 1994; 344: 796-798.
77.Hoffer A: L-dopa: an hallucinogen. Schizophrenia 1970; 2:37, and 1970; 2:127.
78.Hoffer A: Dopamine, noradrenalin and adrenalin metabolism to methylated or chrome indole derivatives: two pathways or one? J Orthomolecular Psychiatry 1985; 14: 262-272.
79.Birkmayer W & Birkmayer GJD: Nicotinamide adenine dinucleotide (NADH): the new approach in the therapy of Parkinson’s disease. Ann Clin Lab Sci 1989; 19: 38-43.
80.Birkmayer JGD, Vrecko C, Volc D & Birkmayer W: Nicotinamide adenine dinucleotide (NADH) - a new therapeutic approach to Parkinson’s disease. Acta Neurol Scand, Suppl. vol. 8, 1993; 146P: 32-35.
81.Birkmayer JGD: Nicotinamide adenine dinucleotide (NADH) the new therapeutic approach for improving dementia of the Alzheimer’s type. Forschungs- und Lehreinrichtung des Birkmayer Instituts fur Parkinsontherapie. Vienna, Austria. Menuco Corp., 350 Fifth Ave., Suite 7509, New York, NY 10118.
82.Birkmayer JGD & Birkmayer W:The coenzyme nicotinamide adenine dinucleotide (NADH) as biological antidepressive agent. Experience with 205 Patients. New Trends in Clinical Neuropharmacology 1991;
5: 19-25 .
83.Schapira AHV, Cooper JM, Dexter D, Clark JB, Jenner P & Marsden CD: Mitochondrial complex I deficiency inParkinson’s disease. J. Neurochem 1990; 54: 823-827.

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)