 |

|
|
|
|
 Back to 1996 3rd Quarter Table of Contents
Back to 1996 3rd Quarter Table of Contents
For over four and a half decades Orthomolecular Medicine has sought to justify its continued existence in the face of hostility from the orthodoxy in Medicine, even though the evidence is overwhelming that it works, often better than the offerings of the orthodoxy. This paper is an attempt to find a new justification for Orthomolecular Medicine, that it is a reflection of the origin and evolution of the Universe. Further, the principal complaints against it are not justifiable in this, the Relativistic-Quantum Universe. IntroductionI became active in Orthomolecular Medicine in January 1974. I felt forced to do so, but have not regretted my involvement at any time since. I knew about Hoffer’s and Osmond’s work on schizophrenia1 since 1956 when my father became involved with them. His role, being in the field of Administration, was to inquire into the administrative aspects of Psychiatry, later evolving into an inquiry into the administrative aspects of medicine as a whole2, not to mention nursing3. I was in high school at the time but was kept informed of progress over the subsequent years as I proceeded through medical school at the University of Glasgow, receiving ample exposure to the conventional view. There was no opportunity nor perceived incentive for me to try Orthomolecular techniques as I worked for two years as a General Practitioner in the East end of the city of Glasgow. I emigrated to Canada in 1970 and have remained in General Practice in Creston ever since. The turning point came with my dissatisfaction with the psychiatric opinions provided by the sole psychiatrist in the region in the early 1970s. The vast majority of patients referred by myself, and other 1. Box 0, 1,000, Northwest Boulevard, Creston, B.C., Can.V0B 1G0 local doctors, returned with the diagnosis of “catatonic schizophrenia” no matter what the situation might actually be. I could not believe this. There had to be something better. I remembered what I had learned through my father, and made contact with Dr. Hoffer who kindly invited me to spend a few days with him at his office in Saskatoon in late 1973. Soon after the first chance came for me to apply what I had learned. By 1976 I had accumulated enough experience to present my preliminary results to an international meeting in Denver in March of that year. I reported that, as a G.P., I could help about 78% of schizophrenic patients to be come symptom-free with orthomolecular techniques. My subsequent experience has been similar, provided that the patients followed the advice given to them. Shortly after, by my early involvement with the dawning Space movement, I began to realize that orthomolecular medicine had freed my mind to take a new approach to many common medical conditions. I realized that this was a new medical paradigm, which, in time, I came to call Extraterrestrial Medicine (ETM). I looked at the known physiological changes experienced by astronauts, better cosmonauts, and applied those changes to the illnesses commonly seen by myself in my practice. It became apparent that most of them could get better if the patients could enter space4. A slight shift of perspective made it clear that ETM was a not merely a subset of orthomolecular medicine, but might actually be its future5. I have continued to reexamine ETM from different viewpoints since and remain satisfied that it may be a valid concept6-11. Despite the experience of many spaceflights afterwards, and the ease by which the predictions of ETM can be disOrthomolecular Medicine in the Universe proved, ETM remains unrefuted as yet12,13. universe. Clearly the universe cannot be Returning to my father, as he younger than they are. The upper limit is looked further and deeper into the fundaabout 20 billion years. mentals of his work, of which the medical The universe is a well-integrated and psychiatric aspects were a very small physical system, its laws and properties part, it became apparent that the concepts being the same wherever we look, even he was developing, the forms of authority, places which cannot have had any contact how decisions are made, how the organiwith each other since a small fraction of a zational structures are built up to make second after the instant of creation. The decisions, how the types of personalities universe is expanding. This is known from have evolved to play roles in society, as measurements of the relationship between summarized in a paper of mine recently14, the distances of galaxies and the rate at might reflect basic properties of the uni-which they are receding from us, as known verse15. Specifically it became harder and since the work of Hubble in the 1920s. harder to conceive of a Universe contain-It is this last which has given us a tool to ing intelligences such as our own which study the early universe. If it is expanding, did not operate along the lines which he then we can work out its history in reverse described. In an analogous fashion it has mathematically, arriving at the idea of the become apparent to me that, over and universe being in a hot, dense state in its ear-above the concepts of ETM, orthomoleculiest eras, as predicted by George Gamow in lar medicine might better reflect the funthe 1940s16. The cosmic background radiadamental properties of the universe better tion is the echo of this state and was also pre-than orthodox medicine. dicted by Gamow. Its discovery founded modern cosmology. Extending the process The Early Evolution of the Universe further has allowed studies of The First Three The universe is very big. It is bigger Minutes 17, taking us to a time within 10-43 than we can know. However powerful our second of the instant of creation. observing instruments can become there Some problems (albeit seeming minute) is an insurmountable barrier to our obserwith inconsistencies between theory and vations. Remembering that when we look observations have focused attention on the ever further out in space we look further era between 10-34 and 10-32 second from crea-back in time, we cannot see beyond the tion. The solution seems to be what has come distance equivalent to the time when the to be called the inflationary era18 during universe was about three hundred thou-which there was an exceptionally rapid ex-sand years old, the transition between pansion of the universe, making it as big as when it was opaque to radiation and trans-was indicated above. parent to radiation. This has been reached As far as the instant of creation itself, by observing the cosmic background ra-that is at present unknowable. But there diation. The probability is that the ob-are two general hypotheses covering that servable universe is very small indeed com-situation. The first is that it happened spon-pared with the total universe. taneously, perhaps as a consequence of the The universe is very old. Unless there inflation theory. The second is that it was is a drastic revolution in atomic physics a deliberate act of some powerful, external changing our understanding of how mat-agency, the creator hypothesis. At the mo-ter behaves and hence how stars evolve, ment, there is no evidence to distinguish the lowermost limit is some 15 billion between the two, and no one can be criti-years. This has been determined by stud-cized for choosing one over the other. ies of the evolution of the globular star clus-What is known is that hydrogen was, ters–the oldest known structures in the and still remains, by far commonest ele-ment born in the early universe. There were whole orders of magnitude lesser quantities of the heavy isotope of Hydro-gen (deuterium), helium-3 and helium-4, lithium-7, and, in even very much lesser quantities, beryllium-7. The temperatures and pressures were too high for any other elements to exist long.19 Then how did the other elements come into being? The Source of Biological MoleculesOrthomolecular medicine is defined, paraphrasing Linus Pauling, as the treat-ment of illness by the provision of the op-timum quantities of molecules which are already present. The existence of those molecules and their coming to the Earth was a staged process. A. Stellar Evolution and NucleosynthesisApart from the hydrogen and lithium mentioned above, none of the elements involved in biological processes existed in the early universe. They had to be created by other means. The key to understand-ing how they came to be lies in the stars of the globular clusters, the earliest bodies to form, as far as we know, as the universe began evolving into the form we know today. In the early spectroscopic studies of the nature of the stars there came to be recognised two general types, Population I and Population II. Population II stars are typical of those in the central bulge of the galaxy, the stellar halo surrounding the galaxy and of the globular clusters. It is possible that the core and halo stars arose in globular clusters which were gravitationally disrupted by the develop-ment of the early galaxy. They are charac-terised by a marked sparcity in their spec-tra of lines corresponding to heavier ele-ments than those mentioned above. Popu-lation I stars are typically those found in the galactic arms and in active star form-ing, H II, regions. They are very much younger and are also characterised by the possession of lines indicating heavier ele-ments in their spectra. Stars can be classi-fied in other ways. Subramanian Chandrasekhar, at the age of 19, set off for Cambridge University from India by steam ship. By the time he had arrived in England he had solved, in general lines, the evolution of stars, the more massive, brighter stars in particular. He derived a limit, now known not surprisingly as the Chandrasekhar Limit, which amounts to 1.44 times the mass of our Sun. Above that limit, a star has to under go that most violent of eruptions, the explosion known as a Type II Supernova. Below that limit stars evolve a great deal less violently. The most powerful tool for studying the evo-lution and fate of stars, en masse and in-dividually, is the Herzsprung-Russell Dia-gram, (Figure 1). This relates the bright-ness to the surface temperature, and is Figure 1. The Herzsprung-Russell Diagram Brightness 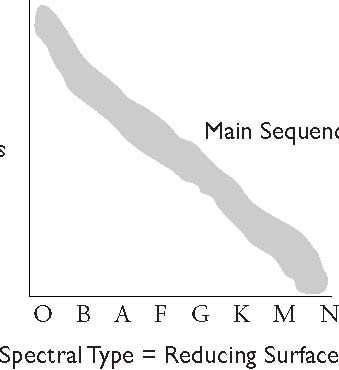  dominated by a gently curving, diagonal band known as the Main Sequence. All stars, Population I or II, massing below or above the Chandrasekhar Limit, have to spend some lesser or greater time on the main sequence, having emerged from the clouds of gas out of which they formed above and to the right of the Main Sequence in the form of T-Tauri stars and migrating into the Main Sequence. When stars form, they do not do so individually but as members of a cluster within a cloud of collapsing gas. As the stars ignite into the T-Tauri stage they blow off the gas unused in star formation. If the originating cloud is very massive and lots of stars are formed, the stars tend to remain bound together, which seems to have been the prevailing situation in the early universe, resulting in globular clus-ters. More recently the clouds seem to be less massive resulting in less gravitationally bound clusters, which tend to disperse. But the masses of the stars which form in any cluster is randomly distributed from the heaviest, O, to the lightest, N, early or late in the universe, in Population I or II stars. The more massive the star the greater the gravitational force on its core, the brighter it is, the faster it burns its nuclear fuel, and the sooner it evolves back off above and to the right of the main sequence again. For the most massive stars this can happen within a few hundred thousand years, for the least tens of billions of years. The stars in each of the globular clus-ters, of which the nearest and most visible example is the Omega Centauri cluster in the southern skies, are presumed to have formed at the same time. There is no evi-dence to the contrary. In no such cluster are there any known examples of massive, bright stars. All of them have suffered their destructive fates billions of years ago. What are now observed are stars of the M and N types, or their counterparts evolv-ing off the Main Sequence as red giants. Only recently have white dwarf stars been detected by the Hubble Telescope in the Orthomolecular Medicine in the Universe globular clusters, and these are the cinders of the bright, massive stars. What role does the Chandrasekhar Limit play in all this? Stars at or below this mass have a less spectacular fate than the ones above. Once they have begun ex-hausting their hydrogen fuel, their cores shrink and heat up to start burning the helium which is the ash of nuclear burn-ing of hydrogen. Because of the much higher, albeit less efficient, energy output, the outer layers of the stars are pushed out-wards and appear red, forming the Red Giant stage of a star’s life. This stage is not simple at all because, as a side effect, a wide variety of subatomic particles are produced. The result is the synthesis of all the elements of the Periodic Table up to the noble gas Argon. This includes carbon, nitrogen, oxygen, fluorine, sodium, magnesium, alu-minium (aluminum to North Americans), silicon, phosphorus and chlorine20. Of course hydrogen and lithium are still present. In other words, some of the most important elements for biology are formed in this fashion, but not all. After helium burning is exhausted in its turn, the stellar core collapses again. The rising heat blows the outer layers of the star off into Space, leaving behind a white dwarf star. A white dwarf star shines not by nu-clear reactions but by the slow radiation of its accumulated energy trapped in the degenerate matter of which it is composed. Eventually, after many billions of years, what is left is a black dwarf. But the uni-verse is too young for any examples of black dwarves to have appeared. The heavier elements form in stars more massive than the Chandrasekhar Limit. everything they do happens faster than in the case of the lighter stars. They quickly exhaust the hydrogen fuel and enter the helium burning stage, forming the above noted elements, and becoming red giant stars. Under the concealing red envelope more spectacular events are starting to hap-pen. Unlike the lighter stars, when the he-lium burning starts to become exhausted, their cores collapse even further, and pro-gressively hotter, burning reactions take place rather like the layers of an onion. In summary the layers of the stellar on-ion are, from outside in, Hydrogen Burn-ing, helium burning, carbon burning, oxy-gen burning21 (by which time the red, outer atmosphere of the star is being blown off, revealing a smaller but very much more lu-minous supergiant star), and silicon burn-ing22 (a term not accepted by all astrophysicists). The “ash” from this last phase is iron predominantly, and iron-like elements. Also mixing in all the layers are the elements up to iron. An important point is that nucleons are most tightly bound in the Iron nucleus, which leads to catastrophe. There is no iron burning. As the iron accumulates, the core continues to collapse because there are no further nuclear reac-tions to hold it up. As it collapses the tem-perature rises, until it reaches the order of about ten billion degrees Kelvin. At this temperature the structure of the Iron nu-cleus breaks down into simple nucleons again, electrons and protons (which almost immediately recombine into neutrons), neutrons, and neutrinos (which are the only particles which can escape)–a reaction which is a net absorber of energy. The core implodes, and then “hardens”. As the im-plosion happens, the layers of the star above the core fall inwards, compress and hit the outer boundary of the hardened core. A shock wave races through the substance of the star, a process which is not as simple as it sounds. When the shock wave reaches the surface, it is so energetic that for about one tenth of a second the dying star out-shines all the stars of a major galaxy put together. A Type II supernova has erupted. In this immense explosion the storm of nucleons is so fierce that all the elements heavier than argon may be synthesized23 and be blown into the interstellar gas in the forms with which we are familiar. This includes such orthomolecularly important elements as potassium, calcium, chromium, manganese, iron and cobalt, copper, zinc, selenium, iodine, gold, mercury, and lead, not to mention immense addi-tional quantities of the elements formed from the evolution of lighter stars. Along with them are formed transplutonian ele-ments which break down long before we can become aware of their presence. Most supernovas leave behind neutron stars as their corpses. A few are so massive that their corpses are in the form of black holes. Type I supernovas, much less violent, oc-cur when a clump of matter falls on to a neutron star or into a black hole. Returning yet again to the globular clus-ters, the formation of the heavy elements began with their early massive stars erupting as supernovas and spreading these elements into interstellar space. No stars hotter than M or N stars exist in any globular clusters. The enriched interstellar gases, compacted by the criss-crossing shockwaves, form clouds out of which new generations of stars ap-pear, a significant proportion of them repeat-ing the cycle of heavy element synthesis. It may be that the Sun, and the planets of its family, are of the fourth generation of this cycle of nucleosynthesis. B. Formation of Pre-biotic MoleculesPerhaps about five billion years ago the pressure wave from a supernova explosion passed through an extensive cloud of gas and dust, triggering localised concentrations within the cloud. This began the sequence of events which brought about the birth of a new cluster of stars. As what seems to be an inevitable part of the process planets (also asteroids and comets) formed along with the stars. Among these planets was the Earth, a hot place under the fierce radia-tion of the early Sun in its T-Tauri stage, inhospitable to life, even to the very chemi-cals from which life could emerge. The young Sun cooled as its nuclear reactions settled into a quasi-steady state and evolved into the Main Sequence as a G5 star. Once it had done so the surface of the primitive earth could begin cooling to the temperature at which the basic Orthomolecular Medicine in the Universe chemicals, from which life could develop, could survive. Yet none of the those chemicals were present on the Earth. They had to be brought to the planet. Where from? As far back as the 1950s Fred Hoyle suggested that they might originate in the cloud of gas and dust out of which the solar system formed,24 a speculation which could not be confirmed until the golden age of radio astronomy began at least a decade later. With access to the radio bands astrono-mers began to find an increasing list of complex molecules in the types of clouds of gas and dust out of which stellar systems form. One such cloud is the familiar M42, the Great Nebula in Orion, a rich star form-ing region. Before star formation actually begins such clouds form excellent environments for the synthesis of increasingly complex molecules. The basic atoms are there. The environment is cold, but star light and ran-dom motion bring the atoms into contact with each other to build the simplest mol-ecules. Similarly the simple molecules come in contact with each other and react to form more complex molecules. The low temperatures make for a low probability for thermal break-up of such molecules. One exceedingly important point not mentioned in the astronomical literature is that the very dust grains which exist in such colossal profusion in the clouds may act as highly effective catalysts. They carry on their surfaces very reactive forms of various metals such as magnesium, cal-cium, chromium, manganese, iron, cobalt, copper, zinc (implicated in the form of zinc based clays as the basis for the start of true biological activity), and selenium — all familiar to orthomolecular physicians. Also of importance are likely to be metals of the Periods 5 and 6 of the Periodic Ta-ble which include such elements as Silver and antimony, platinum (and the platinoid group of catalysts), gold, mercury and lead. As bioactive elements their importance continues today as co-factors for various enzymes, or as poisons. How complex may the molecules be-come? The problem is a technical one. If we do not know what the spectral, specifi-cally radio, signature of a particular mol-ecule might be, we cannot even begin to try to identify it in the interstellar clouds. For example, we do not know the signa-ture of the ring molecule benzene. But the benzene ring seems easy to syn-thesize under the conditions in interstellar clouds, and is the precursor of may other organic compounds, single ring molecules like niacin and niacinamide (two forms of vitamin B3) or the ascorbate radical, and multi-ring compounds like the steroids. For another example, considering the biosynthetic process by which cholesterol is formed biologically from simpler mol-ecules, it is easy to conceive how it , and molecules similar to it, might by formed from various combinations of molecules already identified in interstellar clouds. For similar reasons I believe that most of the monosaccharides, simple fats and oils, amino acids, and the bases later to be incorporated in nucleic acids, were formed in the interstellar clouds. It merely remains to determine how to find them, and then I believe we will find them. Certainly the list of complex chemi-cals found in the rare carbonaceous chondritic type of meteors suggests that this account might be correct, but too of-ten they have been contaminated by the earthly environment to be sure. Such meteors have been found spectroscopically to be identical with one of the classes of asteroids, a class which might include “burned out” comets. The total mass of interstellar clouds is many times the combined masses of the stars and planets which will ultimately condense out of them because much of that mass will be blown away when the stars ignite in their T-Tauri stages, as is still happening in the well-known Pleiades clus-ter. While proportionately a small fraction of the total mass, the accumulated mass of each type of molecule is still very great. In other words there is reason to believe that most, but not all, of the substances im-portant to orthomolecular physicians, or-ganic chemicals and the so-called “trace ele-ments”, pre-existed the very formation of the Earth and were active during this period. Once star formation begins the tem-peratures in the clouds rise and the mol-ecules begin to break down. But the same mechanisms which create the stars and brings about the temperature rise, also cre-ates an environment in which the vulner-able molecules are protected–comets. C. The Bringers of LifeComets have been likened by the as-tronomer Fred Whipple to dirty snowballs. Their principal constituent is water ice, mixed liberally with dust grains and or-ganic chemicals. They are of low density and strength. The familiar appearance of comets, the head and the tail, are due to both the heating effect on the comet by the Sun and the pressure exerted by the Solar Wind. They may have a diameter as little as ten metres or as large as several thousand kilometres, e.g. the twin bodies of Pluto and Charon (now known to be unlike any other planets in the Solar Sys-tem and may be the innermost and largest representatives of the newly discovered Kuiper Belt of comets, named after Gerard Kuiper who first suggested such a disk of comets. They are the physical remnants of the origin of the Solar System, appearing as part of the processes which created the Sun and the planets. By far the majority lie beyond the orbit of Neptune in two im-mense groupings. The outermost is as yet theoretical, named the Oort Cloud (named after Jan Oort who first suggested its presence), a vast halo of tens of trillions of comets whose innermost boundary might be about ten thousand Astronomi-cal Units (an Astronomical Unit is the dis-tance from the Earth to the Sun) out from the Sun. Infrared telescopes have detected halos around other stars which seem to correspond to equivalents to the Oort Cloud. Oort suggested such a cloud as the source of sporadic comets which enter the inner Solar System from any direction, perhaps disturbed from their distant or-bits by a passing star some considerable time ago. In from that, formed into a disk by the gravitational influence of the plan-ets, is the Kuiper Belt as mentioned above. This is the source of the long period com-ets, such as Comet Yakutake which re-cently passed the Earth and has an orbital period of about fifteen thousand years. Equivalents to the Kuiper Belt have also been detected around other stars. There are other comets, the interme-diate and short period comets. An exam-ple of the first is Halley’s Comet, and of the second is Comet Swift-Tuttle which is the source of the Perseid meteor shower seen every 11th, 12th and 13th of August. Both types began as members of either the Oort Cloud or the Kuiper Belt, but, be-cause of gravitational interactions with the planets, Jupiter in particular, have been diverted into such lesser orbits. In the early history of the Solar Sys-tem the comets were far more common. They brought life to the Earth. I do not agree with Hoyle and Wickramasingh in their assertion that they brought living organisms. But what they brought was prodigious quantities of water and the or-ganic compounds from which earthly life originated. The molecules already identi-fied, with difficulty, in comets are listed in Table 1.25 Even though the same rain of comets poured upon the other planets, for local reasons the processes which led to life on the Earth were aborted on them early on, except possibly on Jupiter in some very alien form or under the ice layer of Jupiter’s moon Europa. No signs of the earliest stages of the development of terrestrial life remain, but the first fossil remnants of life on Earth date back to about 3.5 billion years ago. Considering what unlikely combination of Orthomolecular Medicine in the Universe Table 1. Molecules in Comets25
Adapted with kind permission of G.L. Verschuur. Remember that these molecules have been detected in the clouds of gas surrounding the nuclei of the comets and in the tails, all driven off and at least partially degraded by light from the Sun. circumstances lead to the formation of any kind of fossils, it is truly remarkable that such ancient signs of life should have been found at all. As a result it has been esti-mated that life appeared within a hundred million years, i.e. 4.5 billion years ago, of the cooling of the surface of the Earth suf-ficiently to allow the presence of free, liq-uid water–the essential prerequisite to the development of life. For reasons given above I believe that many of the substances familiar to and used by Orthomolecular physicians in their practices arrived on the Earth with the comets. I remind you that as the com-ets were the bringers of life to the Earth, they also are potentially the bringers of death to our species. The impacts of the fragments of Comet Shoemaker-Levy on Jupiter in July 1994 ought to speak unimpeachably to that lesson. The Individual and Disease in a Relativistic-Quantum UniverseHaving linked the tools of orthomo-lecular practice to the origin and evolu-tion of the universe, I find it necessary to consider why the resistance to orthomo-lecular medicine continues. Some time ago I wrote in the following terms:26 “Science is built up around the as-sumption that observations can be made which are divorced from the bias of the observer. Medicine, in particular, although it deals with that most subjective of topics the variability of human beings, aspires to the same standards of objectivity. Is that possible? We try. Unfortunately we may try in particularly harmful ways. For example nearly all general practition-ers, and many specialists, have had deal-ings with such organizations as workers compensation boards, insurance compa-nies, and pension boards over the issue of whether or not a patient is in pain. A so-called independent physician is asked by the organization to give another opinion. And that ‘independent’ physician may in-clude in his/her report the phrase “no ob-jective signs of pain.” How quickly we forget what we are taught in medical school. Pain is a symptom. As such it is entirely subjective perceived as such by the sufferer. A perfect example of this is the pain of migraine. Does anyone seriously doubt that migraine is real?Migraine is, however, acon-dition for which there are no objective signs and no confirmatory tests. But the ‘independent’ physician is vio-lating something even more fundamental. Before I get to that, let’s deal with some-thing even more prevailing as current medical dogma. To be respectable, a medi-cal study has to conform to the standards of the ‘double blind controlled study’. Summarizing, in such studies patients are divided into groups which, because of the numbers involved, hopefully individual variability disappears. To one group a pla-cebo, allegedly an inactive substance, is ad-ministered to eliminate the possibility of a placebo effect–where people respond to a substance by suggestion–making the unproven presumption that all conditions are placebo responsive. To another group is administered the old, standard treat-ment. To a third group the new, and sup-posedly improved, treatment is adminis-tered to see whether it brings about an advance in therapy. Under ‘ideal’ circum-stances, there is a fourth group to whom nothing is administered to see how the natural history of the condition evolves– but this is seldom done. The patients are assigned to the groups according to a code which is, supposedly, only broken at the con-clusion of the pre-set test period. The pur-pose of the code is to remove all observer bias. Again, is that actually possible? Of course there are many criticisms of this sce-nario. The numbers are seldom large enough for proper matching of the groups, because of human individuality and variability. The codes are often broken ahead of time, which is seldom confessed to the medical journals in which the results are published. The pla-cebos are seldom actually inactive. Some-times it becomes obvious, because of other effects by the drugs involved, which patients are getting which active medication. But these are not the main problem which I have with orthodox Medicine’s attempts to be objective. I am an amateur astronomer. As well as trying to keep up with medical ‘literature’–an oxymoron–I also try to keep up with what is happen-ing in modern astronomy. That means having some understanding about the dominating theories of modern physics– the Theory of Relativity and Quantum Theory. Much to my surprise they are both highly relevant to modern medicine’s attempts to be objective. The essence of both the Special and General Theories of Relativity is that every observation entirely depends upon the viewpoint of the observer. The theories specifically deal with the effect of the states of motion, steady motion, ac-celeration, and motion under the influence of gravity (Einstein showing how this was equivalent to acceleration), upon what the observer actually observes. But these were only examples of observer bias. Any altera-tion of the state of the observer altered what was being observed. Einstein’s great conclu-sion was that it was not possible to observe anything objectively. The state of the observer(s) always brought in a bias. Since Relativity has been confirmed to the magni-tude of 10-27 (the order of Planck’s constant), this conclusion has to be granted to be valid even in our day-to-day experience. But Quantum Theory is even more relevant to considerations of medical ob-jectivity. This theory had its origin in the work of James Clark Maxwell, who ex-plained Michael Faraday’s experimental results by a short series of equations. Erwin Schrödinger refined these in his ‘Wave Equations’. These equations had testable consequences which made them the foun-dation of the most successful theory in history, Quantum Theory. Imagine a perfect black body — no such thing occurs in nature. But, if it did exist, how would radiation be absorbed or emitted by it? Common sense tells us that the radiation would be emitted quite ar-bitrarily. Quantum Theory states that it happens in discrete energy states, particles (quanta), mathematically related to each other via the Wave Equations. “That Quantum Theory is right is confirmed by the very existence of transistors, junction diodes, masers, lasers and super conduc-tors. And it allows us to understand what happens to atoms, subatomic particles and energy itself. It even is the basis for all of chemistry as Linus Pauling demonstrated as long ago as 1936 for which he won his first Nobel Prize. Unfortunately it also has some nasty consequences, exemplified by the famous ‘Slit Experiment’. If you have a light source and allow radiation from that source to pass through a single narrow slit to be ob-served on a screen beyond, you get the image of that slit. In other words the light is being transmitted through the slit as particles, traveling in a straight line. If they had been waves traveling through the slit, the image would have been smeared out. Now suppose you send the light through two narrow, parallel slits, the image on the screen is of a series of light and dark bands parallel to each other. This can only hap-pen if the light is not particles at all, but waves interfering with each other — the lines on the screen being called interference fringes. Then suppose you arbitrarily ob-struct one of the slits. Again you see the clear, particle generated image of the slit. Open the obstructed slit and the interfer-ence fringes reappear, reflecting the wave nature of the light. In other words the choices you make determine whether or not you see the light as waves or particles. But you can never see them as both simultane-ously — one of the many consequences of the Heisenberg Uncertainty Principle. Now that’s pretty bad. Modern as-tronomy makes it worse. Quasars, ex-tremely small, but extraordinarily bright objects, have been detected very far away in the universe — billions of light years away. Because they are so far away, their light has taken billions of years to reach us. A few of them appear to be double, twinned. In fact what they have turned out to be is single quasars with massive galaxies lying on the line of sight between us and the quasars. Because of Relativity the light from the quasar is bent around the massive galaxy along two different paths to reach us as two images — gravi-tational lensing. If we study the twin im-ages of the quasar using a photographic plate or other imaging technique then we are observing the light in the form of par-ticles, photons, quanta. But we can also get interference fringes by other tech-niques, such as recombining the images with a prism, effectively using the inter-Orthomolecular Medicine in the Universe vening galaxy as a double slit. But we cannot observe the light simultaneously as photons/quanta, and waves. In other words the choice we make now in how we observe the twin images of the quasar determines how the light passes by the massive, intervening galaxy billions of years ago as particles, or as waves, but never both. This means that the choices we make govern how the universe behaves through all of space and time, and, in turn, the outcome of any observations, including medical. The objection to this is that we seem not to see how our choices affect the uni-verse. It does not accord with common sense. And ‘of course’ this can have no application to what we do in medicine. Of course there was a time when common sense led us to believe that the Earth was flat. That was disproved by Ptolemy. Common sense is no guide to anything. Our choices do alter the state of the universe. Our choices still change what it is we observe. And no coding of the pa-tients in double blind studies can alter that fact that what it is we observe changes ac-cording to the viewpoint of how we ob-serve it. We have changed how the pa-tients respond merely by the very fact of making our observations. The proof lies in the fact that very few double blind controlled studies have ever settled any issue in medicine. Furthermore they appear to conceal the reality of the place of any treatment. So we find ourselves in a conundrum. To find the best treatment for our patients we have to try to be as objective as we can be. Yet the very nature of the universe makes that impossible. What can we do? We can accept the limitations that the Universe imposes upon us. We can accept that every interaction with a patient is a series of N=1, hence the phrase ‘practice of medicine’. And we can pool our accumulated experience with pa-tients, using the tool that we all now ought to be using for our practices, the computer. And we can stop pretending to do things which are inherently impossible.” In other words, orthomolecular medi-cine functions not by following the ac-cepted paradigms of orthodox medicine, but within the constraints of the most powerful theories governing the very ba-sic functioning of the universe. ConclusionI have tried to show how most of the basic substances used by orthomolecular physicians were born as an intrinsic part of the processes by which the Universe was born and evolved. In other words they are truly natural in the deepest sense of the word. While the “toximolecular” agents used and advocated by the orthodox medi-cal establishment are permitted to exist by References
the same processes, it is striking that they do not seem to be available in the crucible of the interstellar clouds, and, hence, can-not be said to be natural. Using the “natu-ral” substances in the subjective arena of individual human beings is compatible with the theories by which the origin and evolu-tion of the universe is studied. No such relationship has been claimed by the ortho-doxy. In other words the medical ortho-doxy is totally out of tune with mainstream science, while orthomolecular medicine is fully compatible with it. Sooner or later main stream medicine will find itself forced to encompass orthomolecular medicine. AIAA/SSI Conference, 1993: 210-215. 12. Miller MK: Space makes strange bed fellows, The Sciences, 1995; 3: 12-15. 13.Barnes-Svarney P: Orbitting space clinics, Longevity, 1991; 2: 81. 14. Paterson ET: Methexis and Extraterrestrial Medicine, Space Manufacturing 10, Proceed-ings of the 12th Princeton/AIAA/SSI Confer-ence, 1995; 176-181. 15.Paterson TT: Personal communication. 16.Gamow G: One two three…infinity. New York, Mentor Books. 1947; 310-313. 17. Weinberg S: The first three minutes, New York. Basic Books. 1977. 18.Kolb EW & Turner MS: Inflation, The Early Universe, Frontiers in Physics, New York. Addison-Welsey. 1990.
CASE FROM THE CENTER Trials and Tribulations of a Three Year OldJames A. Jackson, M.T., (ASCP) C.L.S., Ph.D., B.C.L.D.1 |

This website is managed by Riordan Clinic
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2024c
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
Consult your orthomolecular health care professional for individual guidance on specific health problems.
 Download The Full Text Article in (PDF)
Download The Full Text Article in (PDF)