Removal of Dental Mercury: Often an Effective Treatment for the Very Sensitive Patient
Alfred V. Zamm, MD, FACA, FACP1
Abstract
This study covers 22 patients who had multiple severe sensitivities in that they were extremely intolerant to inhalants (particles and vapours), ingestants (food and chemicals) and their own endogenous, normally occurring yeast (Candida albicans).
The removal of dental mercury ("amalgam") fillings was the single most effective method of improving the health of these patients after other methods were instituted, i.e., avoidance, hyposensitization and nutritional improvement.
Keywords: Mercury, dental amalgam, sensitive, hypersensitive, allergic, food allergy, inhalant allergy, chemical sensitivity, selenium, Candida albicans.
Twenty-two patients who were very sensitive to inhalants (particles and vapours) and ingestants (foods and chemicals) as well as endogenous, normally occurring yeast (Candida albicans) were investigated. The removal of mercury ("amalgam") dental fillings was the single most effective method of improving the health of these patients.
Prior to the removal of the dental mercury, other standard methods of therapy had been employed, i.e., avoidance, nutritional improvement and hyposensitization. These were helpful; however, the extremely sensitive patients often found these means limited in their effectiveness. The process of food avoidance often led to serious nutritional problems in the patients with multiple food intolerances.
The patients selected for dental mercury removal were chosen for the following reasons: (1) Extreme sensitivity
1. 111 Maiden Lane, Kingston, New York 12401.
(2) Other therapeutic modalities had been tried and had not been helpful or practical.
The following is an outline of the therapeutic protocol used prior to considering dental mercury removal:
I. Inhalants
A. Particles
Avoidance and hyposensitization where indicated (sublingual or standard buildup technique if sublingual method not satisfactory).
B. Vapours
1. Avoidance:
A detailed method of avoidance was provided to the patient.1
2. Nutritional improvement:
An attempt was made to strengthen the patient's ability to deal with exposure to chemical vapours by the administration of selenium. I have found that in certain patients selenium may benefit some patients who do not tolerate chemical vapours.2 3 4 5 Fifty mcg. of selenium were administered b.i.d., p.c. In some cases the beneficial results were seen within one to two weeks; in other cases within three months.6 7 In many cases no benefit was noticed.
3. Hyposensitization by the sublingual method:
Often this is effective but of limited use; I have found it less effective than selenium.
II. Ingestants:
A. Foods:
1. Avoidance of individual foods per se
2. Avoidance of related food families if applicable
3. Rotation of foods and/or families, if applicable.
B. Chemicals: Avoidance.
138
Removal of Dental Mercury: Often an Effective Treatment for the Very Sensitive Patient
III. Sensitivity to endogenous yeast (Candida albicans)8 9 10 11 12 13
A. Inhalants:
Avoidance of atmospheric and household fungi, since fungi and yeast often cross-react;
B. Ingestants:
Avoidance of products made by fermentation and yeast/fungi-related substances;
C. Endogenous yeast: Anti-Candida albicans therapy: (a) A diet consisting of the absolute avoidance of manufactured sugar and reduced amount of naturally occurring sugars and starches; (b) Nystatin - orally, topically; (c) Oral Acidophilis bacilli when tolerated and only if reported to be helpful.
Methodology of the Study
Prior to a patient's first visit, he/she is sent a number of questionnaires to be answered at home. Among these questionnaires is the following checklist and instructions: "The attached list of Common Complaints (see Table 1, p. 141) may be useful as a summary of your complaints. Please make a check (•) before those complaints that you feel may have some application to your problem."
After the patient had undergone investigation, treatment and mercury removal and had been discharged, he was sent a photocopy of the original "Common Complaints" questionnaire on which he had previously checked off the symptoms that were present prior to his undergoing treatment. This photocopy was mailed to the patient with the following instructions:
1. How many months has it been since your last mercury fillings were removed? Number of months:_________________
2. Enclosed is a photocopy of a portion of your original history, on which you checked the symptoms you had at your initial visit. Please fill in the information required, as follows: Put a + or a 0 or a - in front of each symptom that you checked off, as follows: + = better, 0 = no change, - = worse.
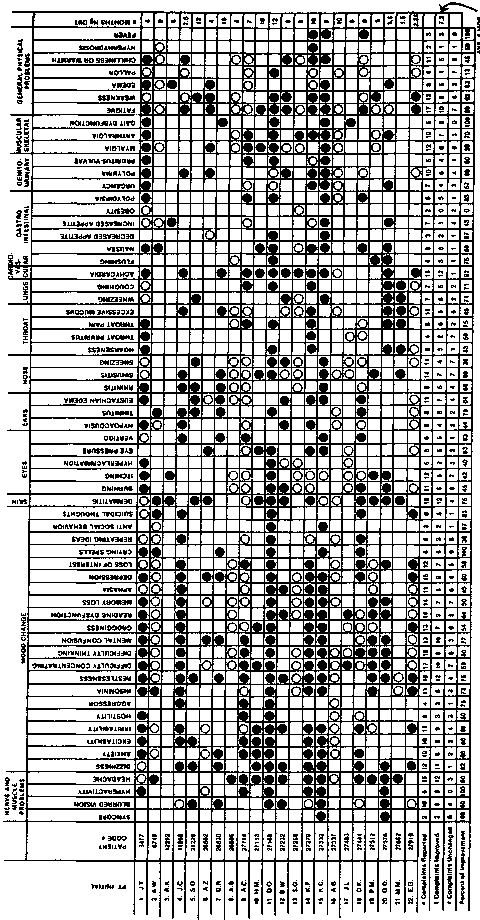
Figure 1 (p. 142) lists the symptoms that the patient complained of prior to being seen for the first time; it also lists the symptoms after the mercury had been
removed and the patients had been discharged. The improvements refer only to that increment and benefit over and above their condition prior to the mercury removal (but after maximum benefit was achieved with previous treatment).
Of 584 symptoms reported, 370 (63%) improved, and 210 (36%) remained unchanged. In regard to symptoms that became worse, there were four such reports out of a total of 584 symptoms reported in all cases, making a percentage of 0.7% that became worse. In all cases of a symptom becoming worse, these were questionable or moderate and without a pattern. No further questioning was done to elicit whether any other factors were operative. The reason for what may be a large percentage of patients showing improvements may be the prior selection process, i.e., these were the sickest patients. The more sensitive patient is the one most likely to note any lessening of metabolic load, however small (in this case, micro-mercurial poisoning.14-25)
It should be emphasized that dental mercury is not the cause of all ills. I have two edentulous patients (no teeth; hence, no mercury fillings!) who have multiple extreme sensitivities.
Removal can be an effective adjunct in treating the very sensitive patient when all else has been tried, but removal does not guarantee a cure or even discernible benefit.
I would like to express my appreciation to Ms. Judith Kistler and Ms. Margaret Davis for their help in the preparation of this manuscript.
References
1. Zamm A, Gannon R: Why your house may endanger your health. New York: Simon & Schuster, 1980; Touchstone Books, 1982.
2. Levine SA, Parker J: Selenium and human chemical hypersensitivities: preliminary findings. Int. J. Biosocial Res. 3:44-47,1982.
3. Levine SA: Oxidants/anti-oxidants and chemical hypersensitivities (Part One) - Ibid 4:51-54, (Part Two) - Ibid 4:102-05, 1983.
4. Levine SA, Reinhardt JG: Biochemical pathology initiated by free radicals, oxidant chemicals, and therapeutic drugs in the etiology of Chemical Hypersensitivity disease./. Orthomol. Psychiat. 12:166-83,1983.
5. Levine SA, Kidd PM: Antioxidant adapta-
139
Journal of Orthomolecular Medicine Vol. 5, No. 3, 1990
don: its role in free radical pathology. San Leandro: Biocurrents Div. of Allergy Research Group, 1985.
6. Zamm A: Observations on use of oral selenium. Letter to the Editor, SCE SCENE, p. 9, October 1983.
7. Parizek J, Ostadalova I: The protective effects of small amounts of Selenite in sublimate intoxication. Experientia 23:142-3, 1967.
8. Zamm A: Chronic urticaria: A practical approach. Cutis, 9:27-37,1972. In: Dickey L (ed.), Clinical Ecology. Springfield: Charles Thomas, pp. 667-701, 1976.
9. Zamm A: Chronic urticaria: The role of food allergy. Cutis, 9:257-270, 1972. In: Dickey L(ed.), Clinical Ecology. Springfield: Charles Thomas, pp. 667-701, 1976.
10. Truss O: Tissue injury induced by Candida albicans: Mental and neurologic manifestations. /. Orthomol. Psychiat., 7:17-37, 1978.
11. Truss O: Restoration of immunologic competence to Candida albicans. /. Orthomol. Psychiat., 9:287-301, 1980.
12. Truss O: The role of Candida albicans in human illness. /. Orthomol. Psychiat., 10:228-38, 1981.
13. Crook W: The Yeast Connection. Jackson, TN: Professional Books, 1983, 1984.
14. Pleva J: Mercury poisoning from dental amalgam./. Orthomol Psychiat. 12:184-93, 1983.
15. Eggleston DW: Effect of dental amalgam and nickel alloys on T-lymphocytes: Preliminary report. /. Prosthetic Dentistry, 51:617-23, 1984.
16. Koller LD: Immunosuppression produced by lead, cadmium, and mercury. Am. J. Vet. Res. 34:1457-58, 1973.
17. Lawrence DA: Heavy metal modulation of lymphocyte activities. In vitro effects of heavy metals on primary humoral immune response. Toxicol. Appl. Pharmacol., 57:349-451, 1981.
18. Zamm A: Letter to the editor, Bio-Probe Newsletter, Orlando, 3:10-12, 1986.
19. Goljan K, Hardy J, Vollmer D, et al: Mercury and dental amalgam: The scientific facts and alternatives. Bio-Probe Manual, 1984.
20.Ziff S: Silver dental fillings: The toxic time bomb; Can the mercury in your dental fillings poison you? New York: Aurora Press, Secon revised edition, 1986.
21. Fasciana GS: Are your dental fillings poisoning you? The hazards of mercury in your mouth — and what you can do about them. New Cannan: Keats Publishing, Inc., 1986.
22. The Bio-Probe Newsletter, Volumes 1:1 to 3:1 incl. Orlando, FL: 1984-86.
23. Ziff S, Ziff M: The hazards of silver/mercury dental fillings. Orlando, FL: Bio-Probe
Newsletter, 1986.
24.Golijan K, Hardy J, Vollmer D, et al: Mercury and Dental Amalgam: The scientific facts and alternatives. Bio-Probe Manual, p. 21, 1985.
25. Zamm A: Mercury and dentistry. Kingston, 1984, i. Reprinted in: Bio-Probe, Vol 2:7 (November) 1985.
140
Removal of Dental Mercury: Often an Effective Treatment for the Very Sensitive Patient
Table 1
Common complaints that the sufferer may not attribute to
a hypersensitivity to foods and/or inhalants.
Nerve and Muscle Problems
|
1. |
Fainting |
|
2. |
Blurred vision |
|
3. |
Unexplained hyperactivity |
|
4. |
Headache |
|
5. |
Dizziness |
|
Mood Changes | |
|
1. |
Unexplained anxiety |
|
2. |
Unwarranted excitability |
|
3. |
Unexplained irritability |
|
4. |
Hostility |
|
5. |
Aggression |
|
6. |
Insomnia |
|
7. |
Restlessness |
|
8. |
Difficulty concentrating |
|
9. |
Difficulty thinking |
|
10 |
Mental confusion |
|
11 |
Grogginess |
|
12. |
Decreased reading comprehension |
|
13. |
Forge tfulness |
|
14. |
Difficulty recalling words |
|
15. |
Depression |
|
16. |
Loss of interest in work or former |
|
activities or hobbies | |
|
17. |
Crying spells |
|
18. |
Tendency for fixed ideas; recycling or |
|
repeating of ideas | |
|
19. |
Antisocial behaviour |
|
20. |
Thoughts of suicide |
Organs and Systems Problems
1. Skin Rashes
Excessive perspiration
2. Eyes Burning Itching Excessive tearing
Feeling of heaviness and pressure within eyes
3. Ears
Dizziness (Meniere's syndrome) Decreased hearing Buzzing in ears (tinnitus) "Plugged" ears (swollen eustachian tubes)
4. Nose
Nasal obstruction
Sinus congestion
Sneezing (Rubbing nose upward is a
sign of allergy)
5. Throat Hoarseness
"Itching" throat (leading to clucking sounds) Sore throat Excessive mucus
6. Lungs Wheezing Coughing
7. Cardiovascular Palpitations Flushing
8. Gastrointestinal Nausea
Loss of appetite
Voracious appetite or sudden weight
gain (5 pounds in 2 days)
Chronic obesity
Excessive thirst
9. Genitourinary Urgent urination Frequent urination Bedwetting Vaginal itching
Excessively painful menstruation
10. Muscular-skeletal Muscle soreness Joint pains Uncertain gait
General Physical Problems
1. Fatigue (physical or mental)
2. Loss of former energy ("getting old")
3. Weakness
4. Edema (swelling)
5. Pallor
6. Inappropriate chilliness or excessive warmth
7. Excessive perspiration without fever
8. Unexplained fevers
Excerpted from the book: Why Your House May Endanger Your Health by Alfred V. Zamm, MD, FACA, FACP, with Robert Gannon. Simon & Schuster, August 1980; Touchstone, May 1982.
141


Journal of Orthomolecular Medicine Vol. 5, No. 3, 1990


142